Hoxha Ariela, Lovisotto Marco, Perin Nicola, Nalesso Federico, Del Prete Dorella, Simioni Paolo
Internal Medicine Unit, Thrombotic and Hemorrhagic Center, Department of Medicine, University of Padua, Padua, Italy.
Nephrology Unit, Department of Medicine, University of Padua, Padua, Italy.
Clin Kidney J. 2024 Oct 7;17(10):sfae302. doi: 10.1093/ckj/sfae302. eCollection 2024 Oct.
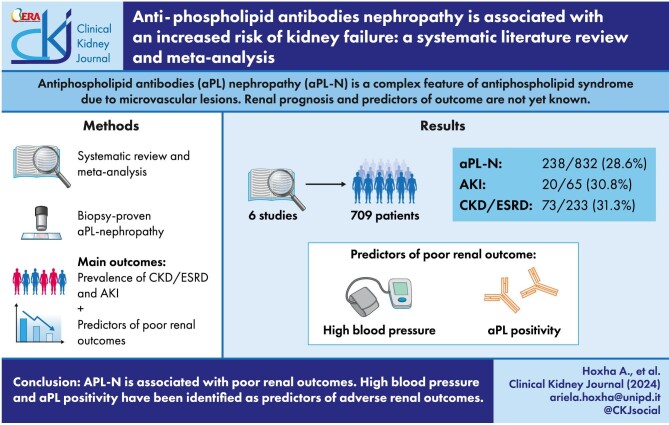
Anti-phospholipid antibodies nephropathy (aPL-N) is a complex feature of anti-phospholipid syndrome due to microvascular lesions. Renal prognosis and predictors of outcome are not yet known.
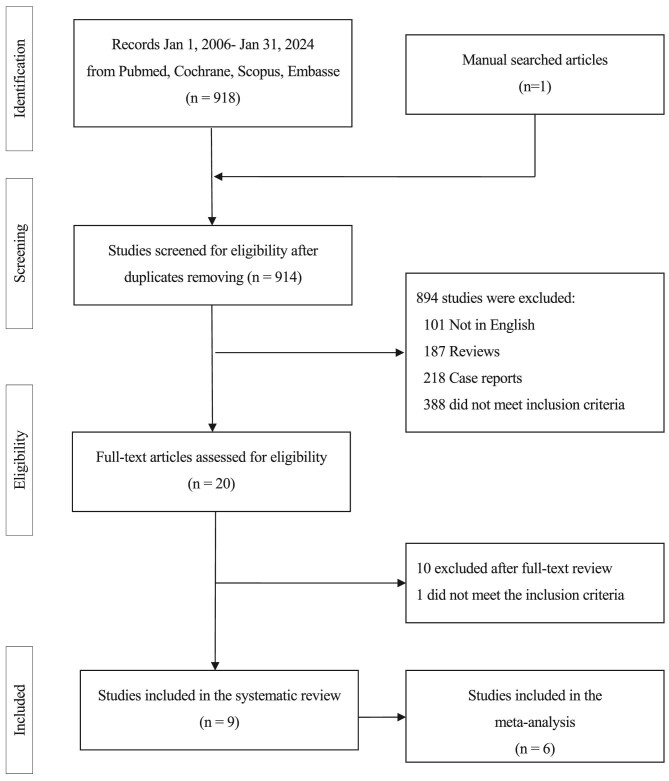
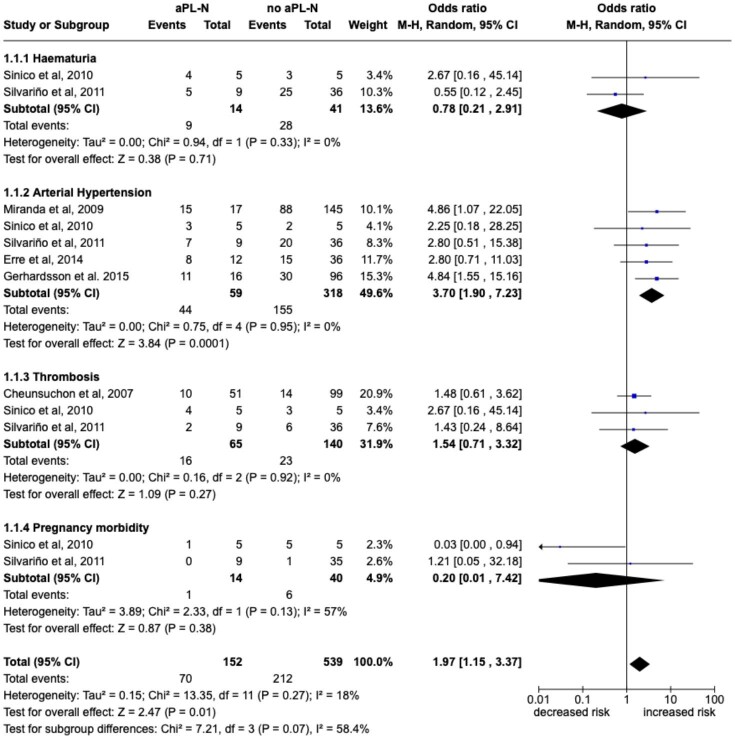
We performed a systematic review of the literature (February 2006-January 2024) using the PubMed, Scopus, Cochrane Library and EMBASE databases. Two reviewers independently conducted literature screening and data extraction in a blinded, standardized manner. A random effects model was used to pool odds ratios (ORs) [with 95% confidence interval (CI)] for the primary analysis, the risk of kidney failure. Subgroup analyses were performed for clinical and laboratory features that predicted renal outcomes. Heterogeneity was assessed by I.
Six records involving 709 patients were included in the meta-analysis. Biopsy-proven aPL-N was found in 238/832 (28.6%) patients. Acute kidney injury (AKI) was present at diagnosis in 20/65 (30.8%), while 73/233 (31.3%) patients with aPL-N developed chronic kidney disease (CKD)/end-stage kidney disease (ESKD) at follow-up. aPL-N was associated with an increased risk of CKD/ESKD [OR 6.89 (95% CI 2.42-19.58)] and AKI [OR 2.97 (95% CI 1-4-6.29)]. Arterial hypertension and positivity for lupus anticoagulant, anti-cardiolipin antibodies and anti-β2 glycoprotein I antibodies were associated with an increased risk of developing aPL-N [OR 3.7 (95% CI 1.9-7.23), OR 4.01 (95% CI 1.88-8.53), OR 2.35 (95% CI 1.31-4.21) and OR 19.2 (95% CI 2.91-125.75), respectively].
aPL-N is associated with poor renal outcomes. High blood pressure and aPL positivity have been identified as predictors of adverse renal outcomes. This up-to-date knowledge on renal outcomes and predictors of renal outcomes in aPL-N enables a personalized follow-up and therapeutic approach.
抗磷脂抗体肾病(aPL-N)是抗磷脂综合征因微血管病变所致的复杂特征。肾脏预后及结局预测因素尚不清楚。
我们使用PubMed、Scopus、Cochrane图书馆和EMBASE数据库对2006年2月至2024年1月的文献进行了系统综述。两名评审员以盲法、标准化方式独立进行文献筛选和数据提取。采用随机效应模型汇总比值比(OR)[95%置信区间(CI)]用于主要分析,即肾衰竭风险。对预测肾脏结局的临床和实验室特征进行亚组分析。通过I评估异质性。
荟萃分析纳入了6项涉及709例患者的记录。活检证实的aPL-N在238/832(28.6%)例患者中被发现。20/65(30.8%)例患者诊断时存在急性肾损伤(AKI),而73/233(31.3%)例aPL-N患者在随访时发展为慢性肾脏病(CKD)/终末期肾病(ESKD)。aPL-N与CKD/ESKD风险增加相关[OR 6.89(95%CI 2.42 - 19.58)]以及AKI风险增加相关[OR 2.97(95%CI 1.4 - 6.29)]。动脉高血压以及狼疮抗凝物、抗心磷脂抗体和抗β2糖蛋白I抗体阳性与发生aPL-N的风险增加相关[分别为OR 3.7(95%CI 1.9 - 7.23)、OR 4.01(95%CI 1.88 - 8.53)、OR 2.35(95%CI 1.31 - 4.21)和OR 19.2(95%CI 2.91 - 125.75)]。
aPL-N与不良肾脏结局相关。高血压和aPL阳性已被确定为不良肾脏结局的预测因素。关于aPL-N肾脏结局及肾脏结局预测因素的这一最新知识有助于采取个性化的随访和治疗方法。