Department of Radiology, XinQiao Hospital of Army Medical University, Chongqing, 400037, China.
Department of Medical imaging, Luzhou People's Hospital, Luzhou, 646000, China.
BMC Pulm Med. 2024 Oct 26;24(1):534. doi: 10.1186/s12890-024-03360-8.
To develop and validate a radiomic model for differentiating pulmonary invasive adenocarcinomas from benign lesions based on follow-up longitudinal CT images.
This is a retrospective study including 336 patients (161 with invasive adenocarcinomas and 175 with benign lesions) who underwent baseline (T0) and follow-up (T1) CT scans from January 2016 to June 2022. The patients were randomized in a 7:3 ratio into training and test sets. Radiomic features were extracted from lesion volumes of interest on longitudinal CT images at T0 and T1. Differences in radiomic features between T1 and T0 were defined as delta-radiomic features. Logistic regression was used to build models based on clinicoradiological (CR), T0, T1, and delta radiomic features and compute signatures. Finally, a nomogram based on the CR, T0, T1 and delta signatures was constructed. Model performance was evaluated for calibration, discrimination, and clinical utility.
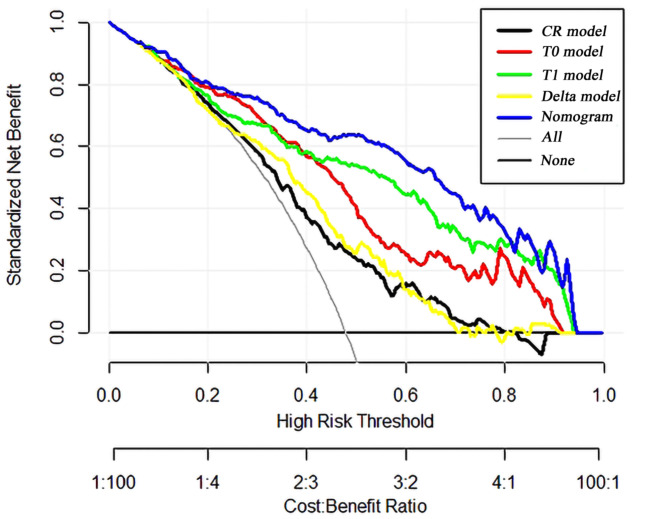
The T1 radiomic model was superior to the other independent models. In the training set, it had an area under the curve (AUC) of 0.858), superior to the CR model (AUC 0.694), the T0 radiomic model (AUC 0.825), and the delta radiomic model (AUC 0.734). In the test set, it had an AUC of 0.817, again outperforming the CR model (AUC 0.578), the T0 radiomic model (AUC 0.789), and the delta radiomic model (AUC 0.647). The nomogram incorporating the CR, T0, T1 and delta signatures showed the best predictive performance in both the training (AUC: 0.906) and test sets (AUC: 0.856), and it exhibited excellent fit with calibration curves. Decision curve analysis provided additional validation of the clinical utility of the nomogram.
A nomogram utilizing radiomic features extracted from longitudinal CT images can enhance the discriminative capability between pulmonary invasive adenocarcinomas and benign lesions.
基于随访纵向 CT 图像,开发并验证一种用于区分肺浸润性腺癌与良性病变的放射组学模型。
这是一项回顾性研究,纳入了 2016 年 1 月至 2022 年 6 月期间接受基线(T0)和随访(T1)CT 扫描的 336 例患者(浸润性腺癌 161 例,良性病变 175 例)。患者按 7:3 的比例随机分为训练集和测试集。从 T0 和 T1 的病变感兴趣区的纵向 CT 图像中提取放射组学特征。T1 和 T0 之间的放射组学特征差异定义为 delta-放射组学特征。采用逻辑回归基于临床放射学(CR)、T0、T1 和 delta 放射组学特征构建模型并计算特征。最后,基于 CR、T0、T1 和 delta 特征构建了列线图。评估模型的校准、判别和临床实用性。
T1 放射组学模型优于其他独立模型。在训练集中,其曲线下面积(AUC)为 0.858,优于 CR 模型(AUC 0.694)、T0 放射组学模型(AUC 0.825)和 delta 放射组学模型(AUC 0.734)。在测试集中,其 AUC 为 0.817,再次优于 CR 模型(AUC 0.578)、T0 放射组学模型(AUC 0.789)和 delta 放射组学模型(AUC 0.647)。纳入 CR、T0、T1 和 delta 特征的列线图在训练集(AUC:0.906)和测试集(AUC:0.856)中均表现出最佳的预测性能,且校准曲线拟合良好。决策曲线分析进一步验证了列线图的临床实用性。
利用纵向 CT 图像提取的放射组学特征构建的列线图可以提高肺浸润性腺癌与良性病变的鉴别能力。