General Surgery Department, Theodor Bilharz Research Institute (TBRI), Giza, Egypt.
Anaesthesiology Department, Theodor Bilharz Research Institute (TBRI), Giza, Egypt.
BMC Surg. 2024 Oct 25;24(1):330. doi: 10.1186/s12893-024-02612-y.
To potentially lessen injuries and associated complications, fluorescence cholangiography has been suggested as a technique for enhancing the visualization and identification of extrahepatic biliary anatomy. The most popular way to administer indocyanine green (ICG) is intravenously, as there is currently little data on ICG injections directly into the gallbladder. In order to visualize extrahepatic biliary anatomy during laparoscopic cholecystectomy (LC), we compared the two different ICG administration techniques. We also examined variations in visualization time, as well as the effectiveness, benefits, and drawbacks of each modality.
In this prospective randomized clinical study, 60 consecutive adult patients with chronic and acute gallbladder disease were included. Our study conducted from 2022 to 2024 in Surgical Department of Theodor Bilharz Research Institute. Thirty patients underwent LC with intravenous ICG administration (IV-ICG), thirty patients received a direct injection of gallbladder through transhepatic ICG (IC-ICG) and Preoperative, intraoperative, and postoperative patient data were examined.
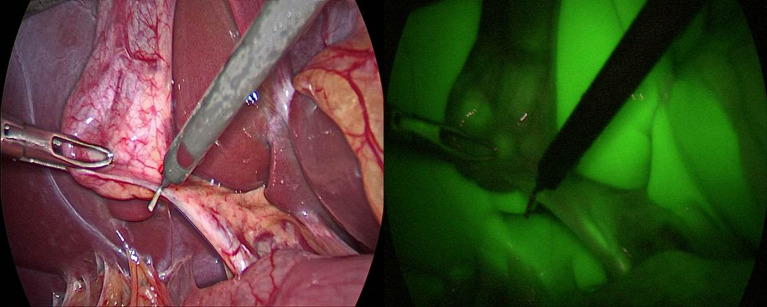
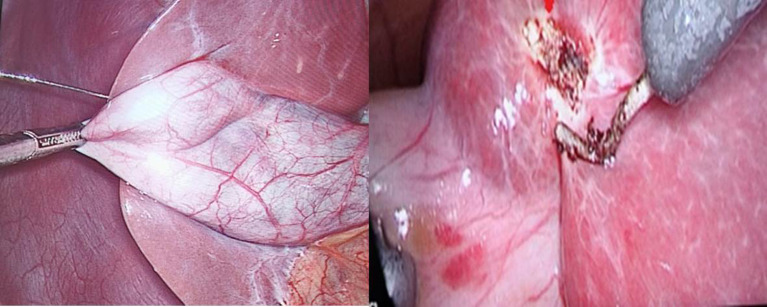
In terms of their perioperative and demographic features, the groups were similar. Without a statistically significant difference, the IV-ICG group's total operating time was less than that of the IC-ICG group (p 0.140). Compared to the transhepatic IC-ICG method, IV-ICG was more accurate in identifying the duodenum and the common hepatic duct (p = 0.029 and p = 0.016, respectively). In the transhepatic IC-ICG and IV-ICG groups, the cystic duct could be identified prior to dissection in 66.6% and 73.3% of cases, respectively, and this increased to 86.6% and 93.3% following dissection. In the transhepatic IC-ICG group, the common bile duct was visible in 93.3% of cases; in the IV-ICG group, it was visible in 90% of cases. Two cases in the IC-ICG group and every case following IV-ICG administration had liver fluorescence (6.6% versus 100%; p < 0.001).
The current study shows that for both administration methods, ICG-fluorescence cholangiography can be useful in identifying the extrahepatic biliary anatomy during Calot's triangle dissection. By avoiding hepatic fluorescence, the transhepatic IC-ICG route can increase the bile duct-to-liver contrast with less expense and no risk of hypersensitivity reactions than the intravenous ICG injection method. We recommend to use both techniques in case of acute cholecystitis with cystic duct obstruction. In cases of liver cirrhosis, we recommend transhepatic IC-ICG as IV-ICG is limited.
为了降低潜在的损伤和相关并发症,荧光胆管造影术已被提议作为增强肝外胆管解剖可视化和识别的技术。目前,关于将吲哚菁绿(ICG)直接注入胆囊的研究数据很少,因此最常见的给药方式是静脉内给药。为了在腹腔镜胆囊切除术(LC)中可视化肝外胆管解剖结构,我们比较了两种不同的 ICG 给药技术。我们还检查了两种技术的可视化时间以及每种方法的有效性、益处和缺点的差异。
本前瞻性随机临床试验纳入了 60 例慢性和急性胆囊疾病的成年患者。我们的研究于 2022 年至 2024 年在 Theodor Bilharz 研究所的外科部门进行。30 例患者接受了静脉内 ICG 给药的 LC(IV-ICG),30 例患者接受了经肝内 ICG 直接注射(IC-ICG)。检查了患者的术前、术中及术后数据。
在围手术期和人口统计学特征方面,两组患者相似。IV-ICG 组的总手术时间与 IC-ICG 组相比无统计学差异(p 0.140)。与经肝内 IC-ICG 方法相比,IV-ICG 更准确地识别了十二指肠和肝总胆管(p=0.029 和 p=0.016)。在经肝内 IC-ICG 和 IV-ICG 组中,在解剖前可以识别胆囊管的病例分别为 66.6%和 73.3%,在解剖后分别增加到 86.6%和 93.3%。在经肝内 IC-ICG 组中,93.3%的病例可见胆总管;在 IV-ICG 组中,90%的病例可见胆总管。IC-ICG 组中有 2 例出现肝脏荧光,而 IV-ICG 组中每例均出现肝脏荧光(6.6%比 100%;p<0.001)。
本研究表明,对于两种给药方式,ICG 荧光胆管造影术均可在 Calot 三角解剖过程中有用地识别肝外胆管解剖结构。与静脉内 ICG 注射方法相比,经肝内 IC-ICG 途径可以避免肝脏荧光,从而提高胆管与肝脏的对比度,且费用更低,无过敏反应风险。我们建议在伴有胆囊管阻塞的急性胆囊炎中同时使用两种技术。对于肝硬化患者,我们建议使用经肝内 IC-ICG 方法,因为 IV-ICG 受到限制。