Sforza Anita, Bonito Andrea, Tiecco Giorgio, Moioli Giovanni, Storti Samuele, Lechiara Marco, Castelli Francesco, Quiros-Roldan Eugenia
Department of Clinical and Experimental Sciences, Unit of Infectious and Tropical Diseases, University of Brescia, ASST Spedali Civili, 25123 Brescia, Italy.
Operating Unit of Infectious and Tropical Diseases, ASST Spedali Civili, 25123 Brescia, Italy.
Microorganisms. 2024 Sep 30;12(10):1989. doi: 10.3390/microorganisms12101989.
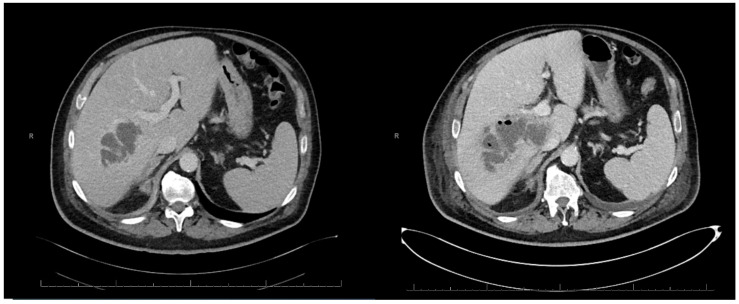
Pyelo-hepatic abscess is a rare complication of upper urinary tract infections (UTIs). We describe a case of polymicrobial pyelo-hepatic abscess in an immunocompetent patient. A 71-year-old male patient with a double-J stent for right ureteral lithiasis was admitted in our Infectious Diseases Department for a pyelo-hepatic abscess. Despite a targeted antibiotic therapy against an extended spectrum betalactamase-negative , the patient did not improve. Further examinations revealed a possible polymicrobial aetiology, including spp. and resistant to piperacillin/tazobactam but sensitive to third-generation cephalosporins. To date, a paucity of articles regarding pyelo-hepatic abscess exist, consisting mostly of case reports. Urinary stones and a ureteral stent indwelling time exceeding 90 days are known risk factors for upper UTIs and for bacterial dissemination in contiguous organs. Pyelo-hepatic abscesses usually involve Gram-negative bacilli, but they can be polymicrobial, including fungi. As a range of factors could limit the efficacy of antibiotics inside an encapsulated lesion and might contribute to the selection of resistant species during treatment, clinicians should be aware of this complication and try to prevent this event by acting on the main modifiable risk factor.
肾盂肝脓肿是上尿路感染(UTIs)的一种罕见并发症。我们描述了一例免疫功能正常患者发生的多微生物性肾盂肝脓肿病例。一名71岁男性患者因右输尿管结石置入双J支架,因肾盂肝脓肿入住我们的传染病科。尽管针对产超广谱β-内酰胺酶阴性菌进行了靶向抗生素治疗,但患者病情并未改善。进一步检查发现可能存在多微生物病因,包括对哌拉西林/他唑巴坦耐药但对第三代头孢菌素敏感的 菌属和 菌属。迄今为止,关于肾盂肝脓肿的文章很少,主要是病例报告。尿路结石和输尿管支架留置时间超过90天是上尿路感染及细菌播散至邻近器官的已知危险因素。肾盂肝脓肿通常涉及革兰氏阴性杆菌,但也可能是多微生物感染,包括真菌。由于一系列因素可能会限制抗生素在包膜病变内的疗效,并可能导致治疗期间耐药菌的产生,临床医生应意识到这种并发症,并应通过控制主要的可改变危险因素来预防这一情况。