Centre for Translational Medicine, Semmelweis University, Üllői Út 26, Budapest, Hungary.
Department of Psychiatry and Psychotherapy, Semmelweis University, Balassa U. 6, Budapest, 1083, Hungary.
Alzheimers Res Ther. 2024 Oct 26;16(1):238. doi: 10.1186/s13195-024-01602-9.
Dementia preventive interventions targeting multiple modifiable risk factors are a promising approach. However, the impact of modifiable risk factors in the presence of beta-amyloid or phosphorylated-tau (p-tau) pathology is unclear.
The objective of the study was to examine the role of modifiable risk factors (vascular factors, depression, and smoking) in the progression to mild cognitive impairment (MCI) or dementia among 434 cognitively unimpaired (CU) and 611 individuals with MCI from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database. Vascular risk factors were summarized with the Cardiovascular Risk Factors, Aging, and Dementia (CAIDE) score, dichotomized into higher versus lower risk. Depression and smoking (yes/no) were categorised according to medical history or current symptoms. Analyses were stratified by beta-amyloid negative (A-) and positive (A +), p-tau negative (T-) and positive (T +), or beta-amyloid and p-tau negative (A-T-) and positive (A + T +) biomarker status. Cox proportional hazard models were adjusted for age, sex, education, baseline MMSE score, baseline hippocampal volume and ApoE4 carrier status.
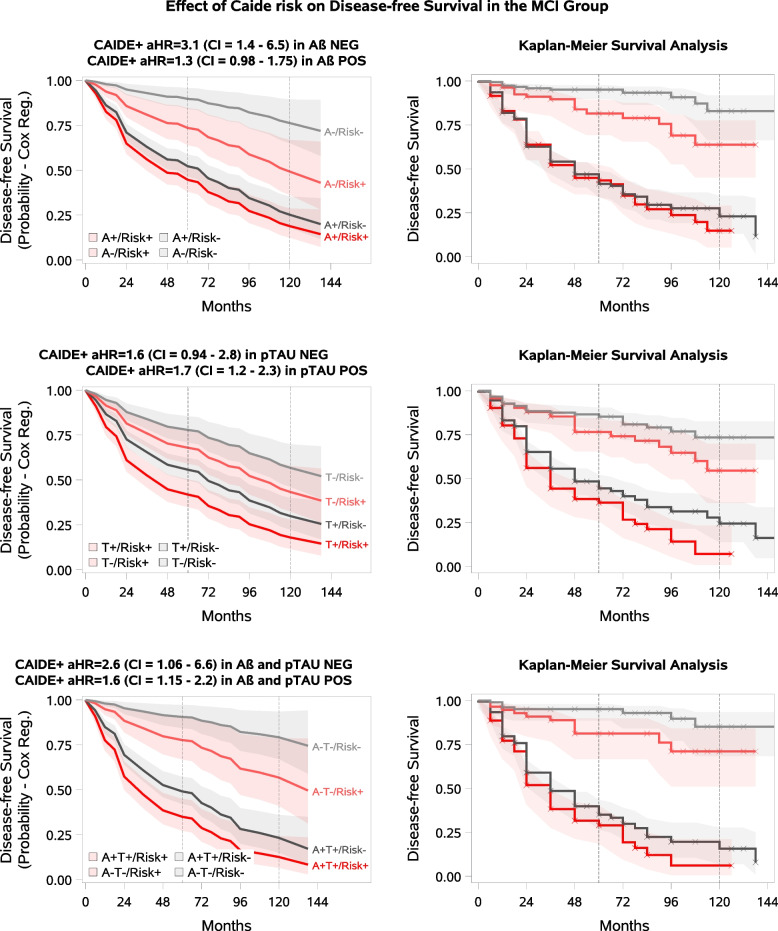
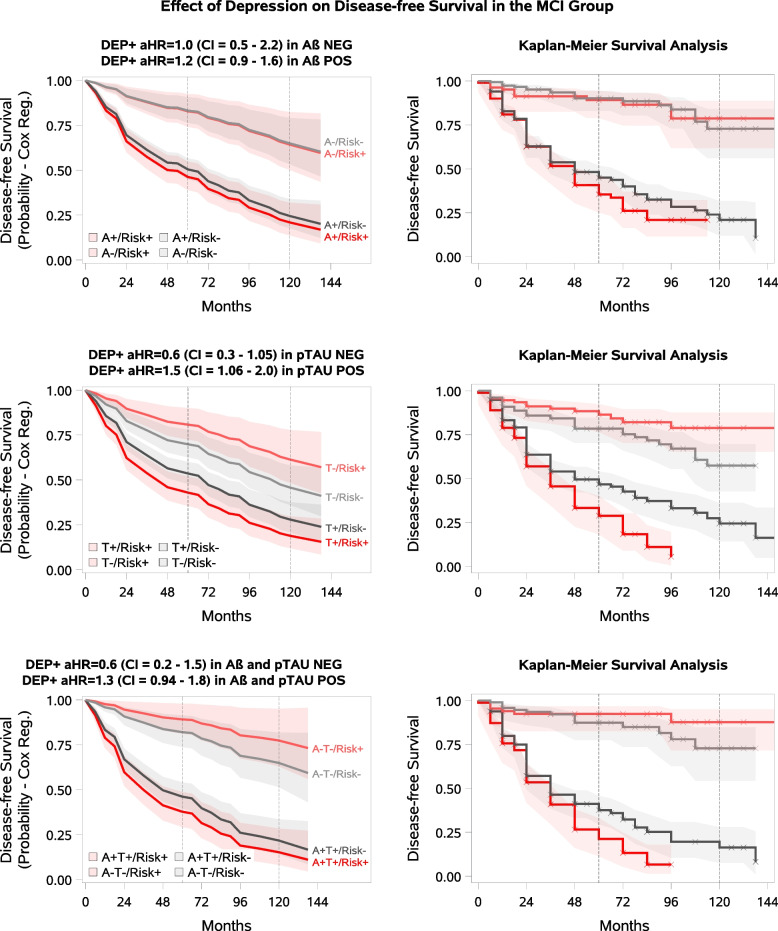
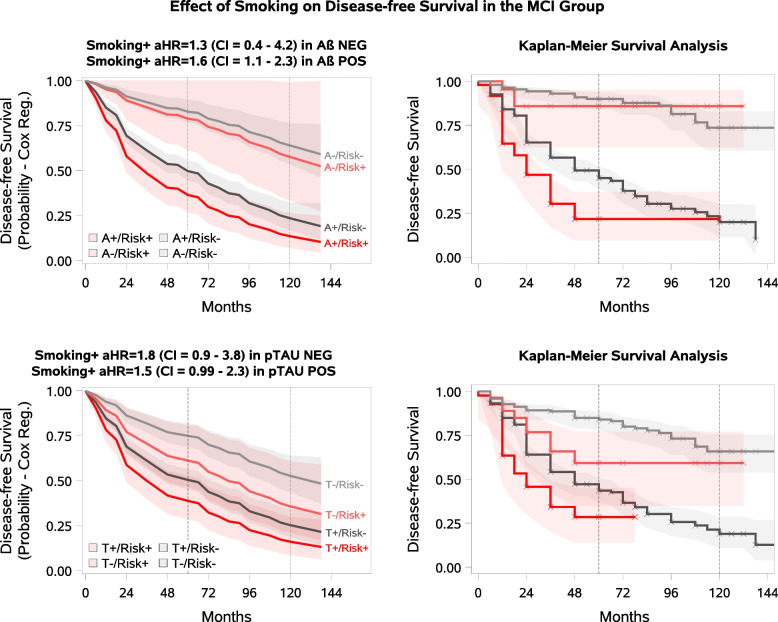
Higher CAIDE score was associated with increased risk of progression to all-cause dementia in most MCI subgroups: adjusted hazard ratios (aHR) [95% CI] were 3.1 [1.43; 6.53] in the A- subgroup, 1.7 [1.20-2.27] in T + , 2.6 [1.06-6.59] in A-T-, and 1.6 [1.15-2.22] in the A + T + subgroup. Smoking (yes/no) was associated with increased dementia aHR in the A + MCI subgroup: 1.6 [1.07-2.34]. Depression increased dementia aHR in the T + MCI subgroup: 1.5 [1.06-2.02]. No significant associations were found in the CU biomarker subgroups.
Addressing modifiable risk factors carries an important potential for reducing the risk of dementia even after the onset of Alzheimer's pathology. Knowledge of biomarker status can further optimize prevention strategies.
针对多个可改变风险因素的痴呆预防干预措施是一种很有前景的方法。然而,在β-淀粉样蛋白或磷酸化 tau(p-tau)病理存在的情况下,可改变风险因素的影响尚不清楚。
本研究的目的是在阿尔茨海默病神经影像学倡议(ADNI)数据库中,检查可改变的风险因素(血管因素、抑郁和吸烟)在 434 名认知正常(CU)和 611 名轻度认知障碍(MCI)患者中向轻度认知障碍(MCI)或痴呆进展的作用。血管危险因素用心血管危险因素、衰老和痴呆(CAIDE)评分来概括,分为高风险和低风险。根据病史或当前症状将抑郁和吸烟(是/否)分为两类。分析根据β-淀粉样蛋白阴性(A-)和阳性(A+)、p-tau 阴性(T-)和阳性(T+)或β-淀粉样蛋白和 p-tau 阴性(A-T-)和阳性(A+T+)生物标志物状态进行分层。Cox 比例风险模型根据年龄、性别、教育、基线 MMSE 评分、基线海马体积和 ApoE4 携带者状态进行调整。
在大多数 MCI 亚组中,较高的 CAIDE 评分与全因痴呆进展的风险增加相关:在 A-亚组中,调整后的风险比(aHR)[95%CI]为 3.1[1.43;6.53],在 T+亚组中为 1.7[1.20-2.27],在 A-T-亚组中为 2.6[1.06-6.59],在 A+T+亚组中为 1.6[1.15-2.22]。在 A+MCI 亚组中,吸烟(是/否)与痴呆 aHR 增加相关:1.6[1.07-2.34]。在 T+MCI 亚组中,抑郁与痴呆 aHR 增加相关:1.5[1.06-2.02]。在 CU 生物标志物亚组中未发现显著相关性。
即使在阿尔茨海默病病理出现后,针对可改变的风险因素进行干预仍具有降低痴呆风险的重要潜力。对生物标志物状态的了解可以进一步优化预防策略。