Fernandez Laura M, São Julião Guilherme P, Santacruz Carlos Cerdan, Renehan Andrew G, Cano-Valderrama Oscar, Beets Geerard L, Azevedo Jose, Lorente Blas F, Rancaño Rocío S, Biondo Sebastiano, Espin-Basany Eloy, Vailati Bruna B, Nilsson Per J, Martling Anna, Van De Velde Cornelis J H, Parvaiz Amjad, Habr-Gama Angelita, Perez Rodrigo O
Colorectal Surgery, Digestive Department, Champalimaud Foundation, Lisbon, Portugal.
Hospital Alemão Oswaldo Cruz, São Paulo, Brazil.
J Clin Oncol. 2025 May 10;43(14):1663-1672. doi: 10.1200/JCO.24.00405. Epub 2024 Oct 28.
Organ preservation has become an attractive alternative to surgery (total mesorectal excision [TME]) among patients with rectal cancer after neoadjuvant therapy who achieve a clinical complete response (cCR). Nearly 30% of these patients will develop local regrowth (LR). Although salvage resection is frequently feasible, there may be an increased risk for development of subsequent distant metastases (DM). The aim of this study is to compare the risk of DM between patients with LR after Watch and Wait (WW) and patients with near-complete pathologic response (nPCR) managed by TME at the time of reassessment of response.
Data from patients enrolled in the International Watch & Wait Database (IWWD) with cCR managed by WW and subsequent LR were compared with patients managed by TME (with ≤10% cancer cells-nPCR) from the Spanish Rectal Cancer Project (VIKINGO project). The primary end point was DM-free survival at 3 years from decision to WW or TME. The secondary end point was possible risk factors associated with DM.
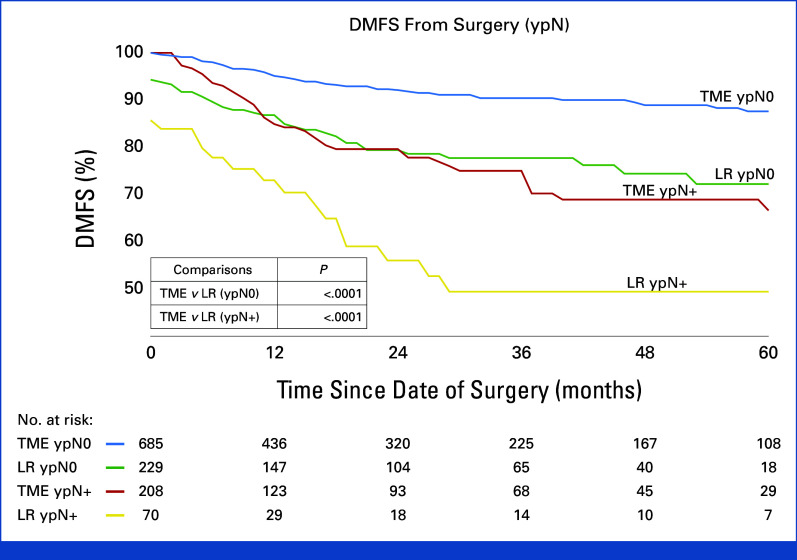
Five hundred and eight patients with LR were compared with 893 patients with near-complete response after TME. Overall, DM rate was significantly higher among LRs (22.8% 10.2%; ≤ .001). Independent risk factors for DM included LR ( TME at reassessment; = .001), ypT3-4 status ( = .016), and ypN+ status ( = .001) at the time of surgery. 3-year DM-free survival was significantly worse for patients with LR (75% 87%; = .001). When stratified for pathologic stage, patients with LR did significantly worse through all stages ( ≤ .009).
Patients with LR appear to have a higher risk for subsequent DM development than patients with nPCR managed by TME at restaging irrespective of final pathology. Leaving the primary undetectable tumor in situ until development of LR may result in worse oncologic outcomes.
对于接受新辅助治疗后达到临床完全缓解(cCR)的直肠癌患者,器官保留已成为手术(全直肠系膜切除术 [TME])之外颇具吸引力的替代方案。这些患者中近30%会出现局部复发(LR)。尽管挽救性切除通常可行,但后续发生远处转移(DM)的风险可能会增加。本研究的目的是比较观察等待(WW)后出现LR的患者与重新评估反应时接受TME治疗且有接近完全病理反应(nPCR)的患者发生DM的风险。
将国际观察等待数据库(IWWD)中接受WW治疗且达到cCR并随后出现LR的患者数据,与西班牙直肠癌项目(VIKINGO项目)中接受TME治疗(癌细胞≤10% - nPCR)的患者数据进行比较。主要终点是从决定进行WW或TME起3年的无远处转移生存期。次要终点是与DM相关的可能危险因素。
将508例出现LR的患者与893例TME后接近完全缓解的患者进行比较。总体而言,LR患者的DM发生率显著更高(22.8%对10.2%;P≤.001)。DM的独立危险因素包括LR(重新评估时未行TME;P = .001)、手术时的ypT3 - 4状态(P = .016)和ypN + 状态(P = .001)。出现LR的患者3年无远处转移生存期明显更差(75%对87%;P = .001)。按病理分期分层时,LR患者在所有分期的情况均明显更差(P≤.009)。
无论最终病理情况如何,与重新分期时接受TME治疗且有nPCR的患者相比,出现LR的患者后续发生DM的风险似乎更高。将原发不可检测的肿瘤原位保留至出现LR可能会导致更差的肿瘤学结局。