Department of Anesthesiology and Department of Medicine, Critical Care Division, Centre Hospitalier de l'Université de Montréal, Montréal, Québec, Canada.
Department of Anesthesiology and Pain Medicine, Université de Montréal, Montréal, Québec, Canada.
JAMA Netw Open. 2024 Nov 4;7(11):e2442361. doi: 10.1001/jamanetworkopen.2024.42361.
In patients with acute myocardial infarction (MI), limited physiologic adaptation to acute anemia might lead to greater benefit from a liberal red blood cell (RBC) transfusion strategy. Data on such a possible benefit are lacking.
To compare acute anemia with chronic anemia and post-MI outcomes and estimate the differential effect of a restrictive RBC transfusion strategy compared with a liberal strategy on post-MI outcomes according to anemia acuity.
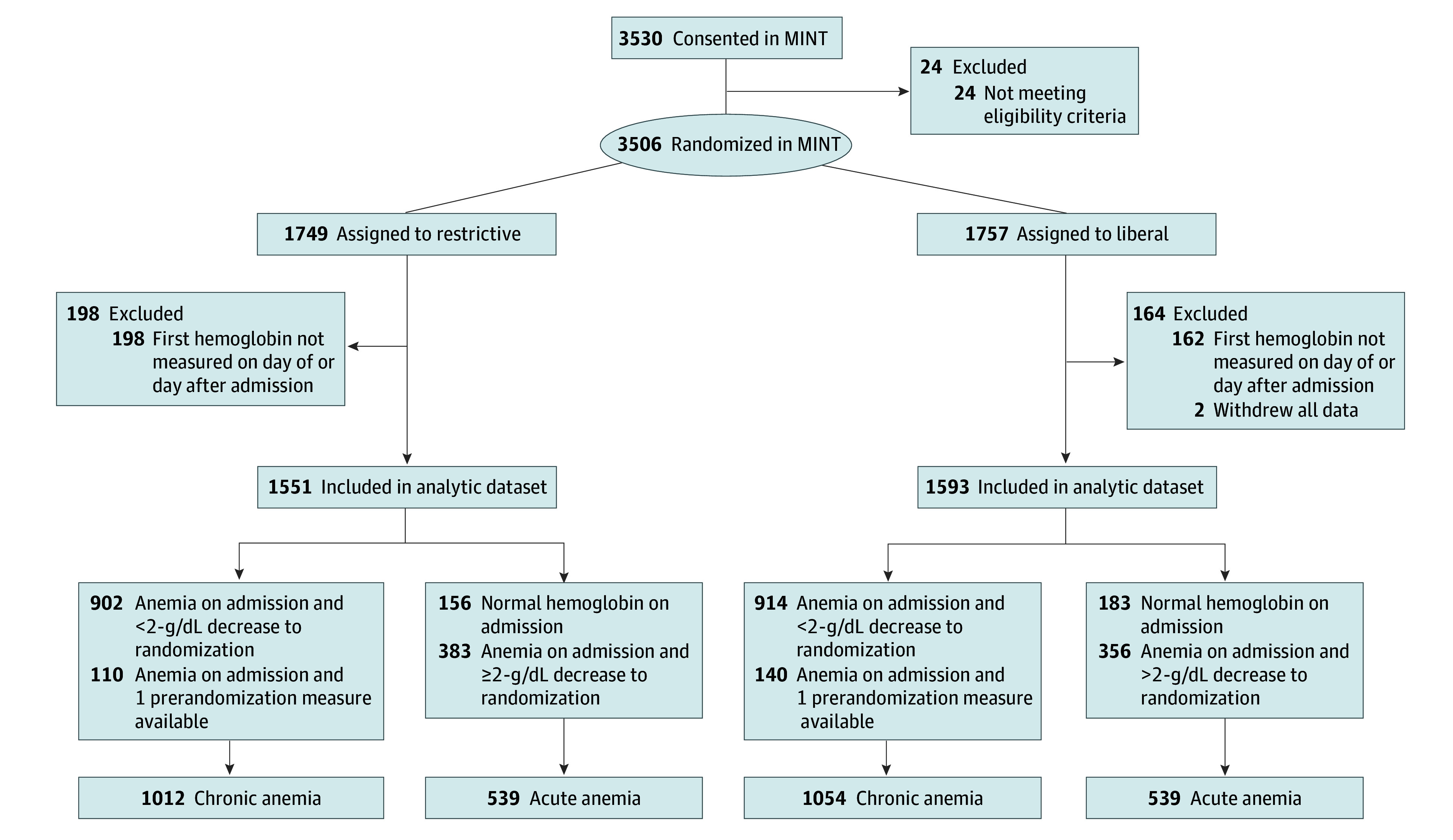
DESIGN, SETTING, AND PARTICIPANTS: A prespecified subgroup analysis of the Myocardial Ischemia and Transfusion (MINT) multicenter randomized clinical trial was conducted in 126 hospitals in 6 countries between April 26, 2017, and April 14, 2023, with 30-day follow-up and blinded adjudication of the primary outcome. The analysis included 3144 of 3504 MINT participants (89.7%) with acute MI, a hemoglobin (Hb) level less than 10 g/dL at randomization, and a first Hb measurement available on the day of or the day following hospital admission.
The MINT trial randomized participants to a restrictive (Hb <7-8 g/dL) or liberal (Hb <10 g/dL) RBC transfusion strategy. Acute anemia was defined as having a first Hb value greater than 13 g/dL (men) or 12 g/dL (women), or as having a decrease greater than or equal to 2 g/dL between the first Hb measurement and measurement at randomization. Other Hb levels were categorized as chronic anemia.
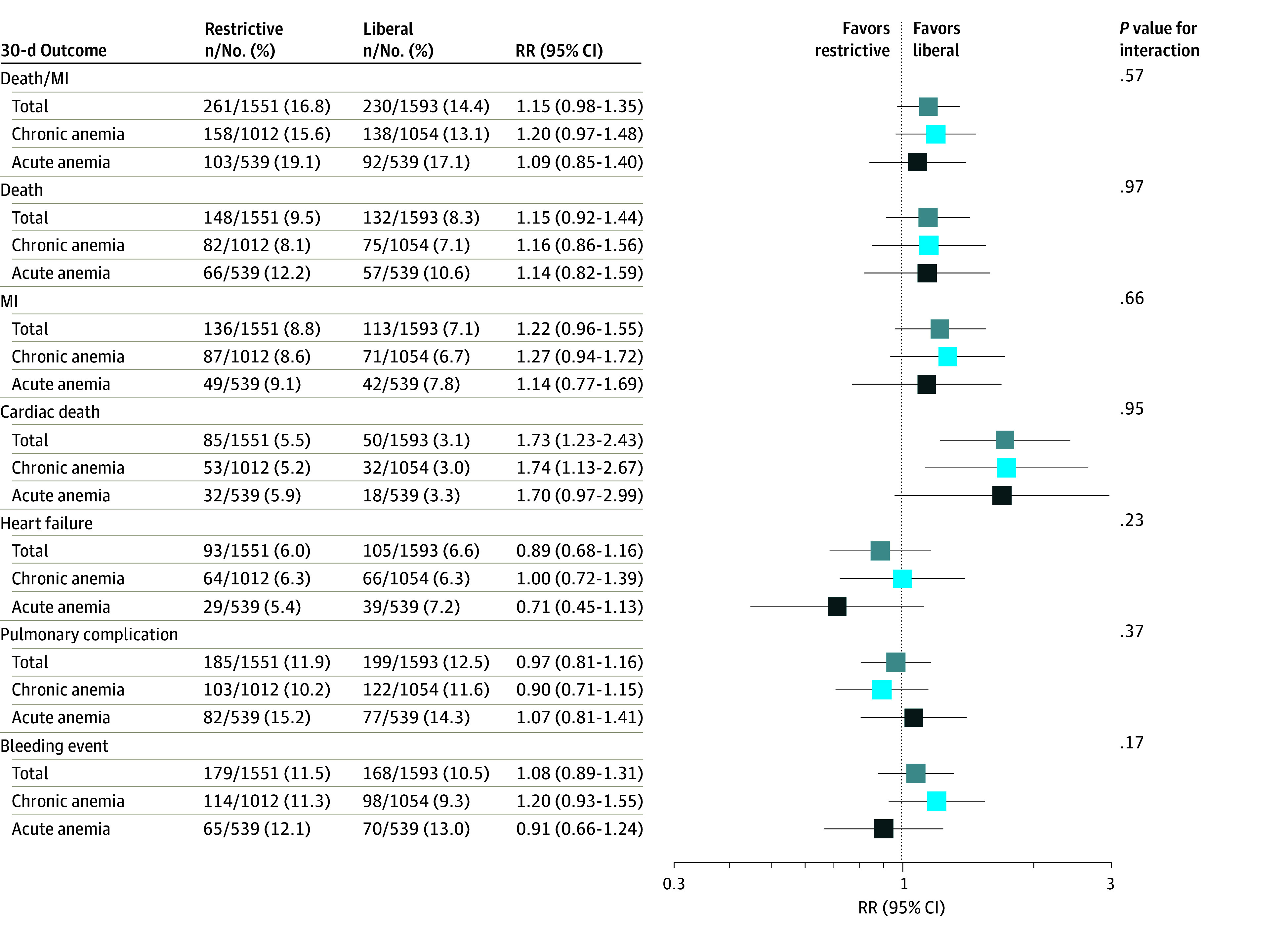
The primary outcome was a composite of death or recurrent MI up to 30 days after randomization. Secondary outcomes were death, recurrent MI, cardiac death, heart failure, pulmonary complications, and major bleeding events. Intention-to-treat analysis was performed.
Among 3144 included participants (mean [SD] age, 72.3 [11.6] years; 1715 [54.5%] male; 1307 [41.6%] with type 1 MI), 1078 [34.3%]) had acute anemia. Acute anemia was associated with an increased risk of death or recurrent MI (adjusted risk ratio, 1.25; 95% CI, 1.05-1.48). The effect of a restrictive RBC transfusion strategy compared with a liberal strategy was similar for participants with either acute or chronic anemia for all outcomes.
In this secondary analysis of the MINT trial, acute anemia was associated with less favorable post-MI outcomes than chronic anemia but did not modify the effects of the randomized transfusion strategy. In patients with anemia and MI, the acuity of anemia should not influence the choice of transfusion trigger.
ClinicalTrials.gov Identifier: NCT02981407.
在急性心肌梗死 (MI) 患者中,急性贫血时的生理适应性有限,可能会从更自由的红细胞 (RBC) 输血策略中获得更大的益处。缺乏关于这种可能益处的数据。
比较急性贫血与慢性贫血以及 MI 后结局,并根据贫血严重程度,估计限制性 RBC 输血策略与自由策略对 MI 后结局的差异影响。
设计、地点和参与者:对 Myocardial Ischemia and Transfusion (MINT) 多中心随机临床试验的预设亚组分析在 6 个国家的 126 家医院进行,于 2017 年 4 月 26 日至 2023 年 4 月 14 日进行,30 天随访,并对主要结局进行盲法裁决。分析纳入了 3504 名 MINT 参与者(89.7%)中的 3144 名,他们在随机分组时有急性 MI,血红蛋白(Hb)水平<10 g/dL,并且在入院当天或入院后第二天有首次 Hb 测量值。
MINT 试验将参与者随机分为限制性(Hb <7-8 g/dL)或自由性(Hb <10 g/dL)RBC 输血策略。急性贫血定义为首次 Hb 值大于 13 g/dL(男性)或 12 g/dL(女性),或首次 Hb 测量值与随机分组时的测量值相比下降≥2 g/dL。其他 Hb 水平被归类为慢性贫血。
主要结局是随机分组后 30 天内死亡或复发性 MI 的复合结局。次要结局是死亡、复发性 MI、心源性死亡、心力衰竭、肺部并发症和大出血事件。采用意向治疗分析。
在 3144 名纳入的参与者中(平均[标准差]年龄,72.3[11.6]岁;1715[54.5%]为男性;1307[41.6%]为 1 型 MI),有 1078 名(34.3%)参与者患有急性贫血。急性贫血与死亡或复发性 MI 的风险增加相关(调整风险比,1.25;95%CI,1.05-1.48)。对于所有结局,与限制性 RBC 输血策略相比,自由性 RBC 输血策略在急性或慢性贫血患者中的效果相似。
在 MINT 试验的这项二次分析中,急性贫血与 MI 后预后较差相关,而慢性贫血则相反,但不影响随机输血策略的效果。在贫血和 MI 的患者中,贫血的严重程度不应影响输血触发的选择。
ClinicalTrials.gov 标识符:NCT02981407。