Université de Paris, AP-HP, French Alliance for Cardiovascular Trials (FACT), INSERM U1148, Paris, France.
Àrea del Medicament Hospital Clínic of Barcelona, University of Barcelona, Barcelona, Spain.
Clin Cardiol. 2021 Feb;44(2):143-150. doi: 10.1002/clc.23453. Epub 2021 Jan 6.
Anemia is common in patients with acute myocardial infarction (AMI), and is an independent predictor of mortality. The optimal transfusion strategy in these patients is unclear.
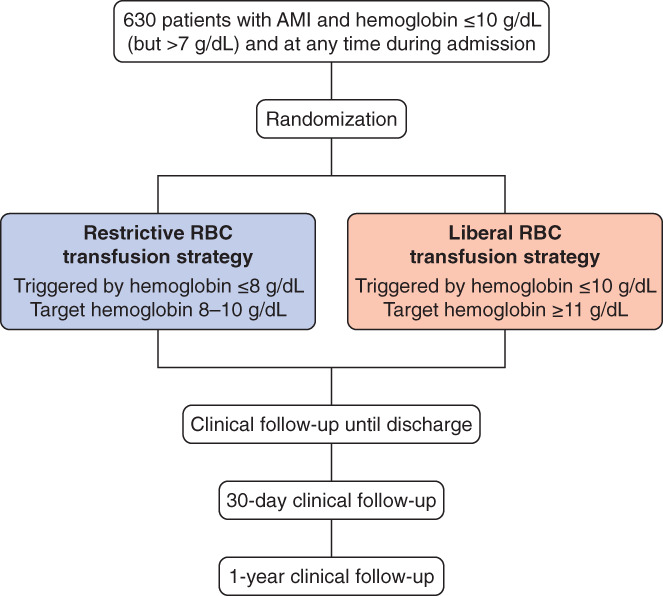
We hypothesized that a "restrictive" transfusion strategy (triggered by hemoglobin ≤8 g/dL) is clinically noninferior to a "liberal" transfusion strategy (triggered by hemoglobin ≤10 g/dL), but is less costly.
REALITY is an international, randomized, multicenter, open-label trial comparing a restrictive vs a liberal transfusion strategy in patients with AMI and anemia. The primary outcome is the incremental cost-effectiveness ratio (ICER) at 30 days, using the primary composite clinical outcome of major adverse cardiovascular events (MACE; comprising all-cause death, nonfatal stroke, nonfatal recurrent myocardial infarction, or emergency revascularization prompted by ischemia) as the effectiveness criterion. Secondary outcomes include the ICER at 1 year, and MACE (and its components) at 30 days and at 1 year.
The trial aimed to enroll 630 patients. Based on estimated event rates of 11% in the restrictive group and 15% in the liberal group, this number will provide 80% power to demonstrate clinical noninferiority of the restrictive group, with a noninferiority margin corresponding to a relative risk equal to 1.25. The sample size will also provide 80% power to show the cost-effectiveness of the restrictive strategy at a threshold of €50 000 per quality-adjusted life year.
REALITY will provide important guidance on the management of patients with AMI and anemia.
贫血在急性心肌梗死(AMI)患者中很常见,是死亡的独立预测因素。这些患者的最佳输血策略尚不清楚。
我们假设“限制”输血策略(血红蛋白≤8 g/dL 时触发)在临床上并不逊于“宽松”输血策略(血红蛋白≤10 g/dL 时触发),但成本更低。
REALITY 是一项国际、随机、多中心、开放性临床试验,比较 AMI 合并贫血患者的限制性与宽松性输血策略。主要结局是 30 天时的增量成本效益比(ICER),使用主要复合临床结局主要不良心血管事件(MACE;包括全因死亡、非致死性卒、非致死性复发性心肌梗死或缺血引起的紧急血运重建)作为有效性标准。次要结局包括 1 年时的 ICER,以及 30 天和 1 年时的 MACE(及其各组成部分)。
该试验旨在纳入 630 例患者。根据限制性组和宽松组的估计事件发生率分别为 11%和 15%,该数量将提供 80%的效能,以证明限制性组在临床上不劣于宽松组,非劣效性边界对应于相对风险等于 1.25。该样本量还将提供 80%的效能,以显示限制性策略在每质量调整生命年 50000 欧元的阈值下的成本效益。
REALITY 将为 AMI 和贫血患者的治疗提供重要指导。