Gregg Justin R, Newcomb Lisa, Wu Ranran, Dennison Jennifer, Davis John W, Pettaway Curtis, Pisters Louis, Ward John F, Chapin Brian F, Chéry Lisly, Urkmez Ahmet, Fang Andrew M, Higgason Noel, Troncoso Patricia, Daniel Carrie R, Logothetis Christopher, Thompson Timothy C, Hahn Andrew W, Liu Menghan, Zheng Yingye, Lin Dan W, Hanash Samir, Irajizad Ehsan, Fahrmann Johannes
The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX, 77030, US.
University of Washington and Fred Hutchinson Cancer Center, 1100 Fairview Ave N, Seattle, WA, 98109, US.
Biomark Res. 2024 Nov 9;12(1):134. doi: 10.1186/s40364-024-00678-7.
We previously reported that increases in circulating sphingolipids are associated with elevated risk of biopsy Gleason grade group (GG) upgrading in men on Active Surveillance (AS) for prostate cancer. Here, we aimed to validate these findings and establish a blood-based sphingolipid biomarker panel for identifying men on AS who are at high-risk of biopsy GG upgrading.
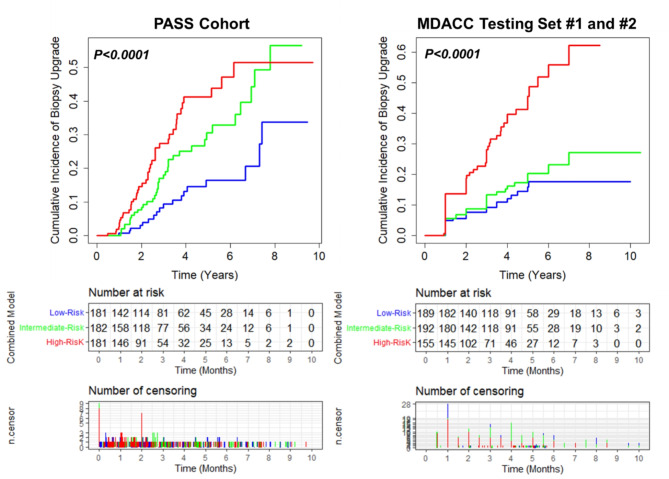
Men diagnosed with low- or intermediate-risk prostate cancer in one of two AS cohorts (CANARY PASS and MDACC) were followed for GG upgrading after diagnostic and confirmatory biopsy. The PASS cohort consisted of 544 patients whereas the MDACC Cohort consisted of 697 patients. The number of patients with GG upgrading during course of study follow-up in the PASS and MDACC cohorts were 98 (17.7%) and 133 (19.1%), respectively. Plasmas collected prior to confirmatory biopsy were used for mass spectrometry-based quantitation of 87 unique sphingolipid species. A neural network layer based on 21 sphingolipids was developed in the CANARY PASS cohort for predicting biopsy GG upgrading. Tertile-based thresholds for low-, intermediate-, and high-risk strata were subsequently developed for the sphingolipid panel as well as a model that combined the sphingolipid panel with PSA density and rate of core positivity on diagnostic biopsy. The resultant models and risk thresholds for GG upgrading were validated in the MDACC cohort. Performance was assessed using Cox proportional hazard models, C-index, AUC, and cumulative incidence curves.
The sphingolipid panel had a HR (per unit standard deviation increase) of 1.36 (95% CI: 1.07-1.70) and 1.35 (95% CI: 1.11-1.64) for predicting GG biopsy upgrading in the PASS and MDACC cohort, respectively. The model that combined the sphingolipid panel with PSA density and rate of core positivity achieved a HR of 1.63 (95% CI: 1.33-2.00) and 1.44 (1.25-1.66), respectively. Tertile-based thresholds, established in the PASS cohort, were applied to the independent MDACC cohort. Compared to the low-risk group, MDACC patients in the high-risk strata had a GG biopsy upgrade HR of 3.65 (95% CI: 2.21-6.02), capturing 50% of the patients that had biopsy upgrading during study follow-up.
The sphingolipid panel is independently associated with GG biopsy upgrading among men in two independent AS cohorts who have previously undergone diagnostic and confirmatory biopsy. The sphingolipid panel, together with clinical factors, provides a potential means for risk stratification to better guide clinical management of men on AS.
我们之前报道过,循环鞘脂水平升高与接受前列腺癌主动监测(AS)的男性活检Gleason分级组(GG)升级风险增加有关。在此,我们旨在验证这些发现,并建立一个基于血液的鞘脂生物标志物面板,以识别接受AS且活检GG升级风险高的男性。
在两个AS队列(CANARY PASS和MDACC)之一中被诊断为低风险或中风险前列腺癌的男性在诊断性和确诊性活检后接受GG升级情况的随访。PASS队列由544例患者组成,而MDACC队列由697例患者组成。在PASS和MDACC队列的研究随访过程中,GG升级的患者数量分别为98例(17.7%)和133例(19.1%)。在确诊性活检前采集的血浆用于基于质谱的87种独特鞘脂种类的定量分析。在CANARY PASS队列中开发了一个基于21种鞘脂的神经网络层,用于预测活检GG升级。随后为鞘脂面板以及将鞘脂面板与PSA密度和诊断性活检时的核心阳性率相结合的模型制定了基于三分位数的低、中、高风险分层阈值。所得的GG升级模型和风险阈值在MDACC队列中进行了验证。使用Cox比例风险模型、C指数、AUC和累积发病率曲线评估性能。
鞘脂面板在PASS和MDACC队列中预测GG活检升级的HR(每单位标准差增加)分别为1.36(95%CI:1.07 - 1.70)和1.35(95%CI:1.11 - 1.64)。将鞘脂面板与PSA密度和核心阳性率相结合的模型的HR分别为1.63(95%CI:1.33 - 2.00)和1.44(1.25 - 1.66)。在PASS队列中建立的基于三分位数的阈值应用于独立的MDACC队列。与低风险组相比,MDACC队列中高风险分层的患者活检GG升级的HR为3.65(95%CI:2.