Zhou Ning, Zhang Kui, Qiao Bokang, Chen Cong, Guo Xiaobo, Fu Wei, Zheng Jubing, Du Jie, Dong Ran
Coronary Artery Disease Surgical Center, Beijing Anzhen Hospital, Capital Medical University, Chaoyang District, China.
Department of Cardiac Surgery, Beijing Anzhen Hopital, Capital Medical University, Beijing, China.
Front Cardiovasc Med. 2024 Nov 1;11:1470987. doi: 10.3389/fcvm.2024.1470987. eCollection 2024.
Accurately assessing the postoperative mortality and rehospitalization for heart failure risks in patients undergoing mitral valve repair surgery is of significant importance for individualized medical strategies.
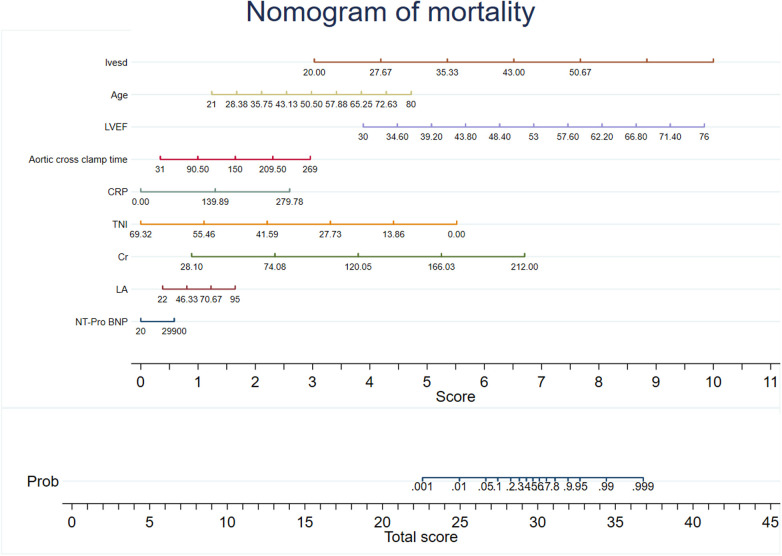
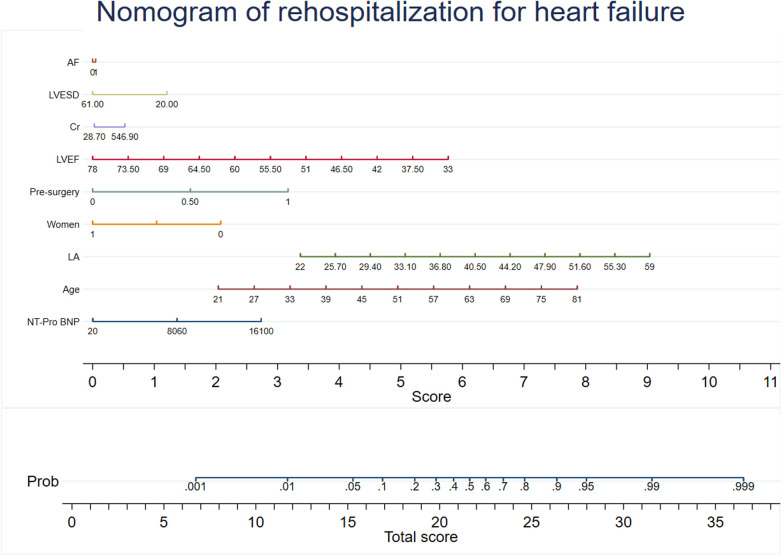
We sought to develop and validate a risk assessment system for the prediction of mortality and rehospitalization for heart failure.
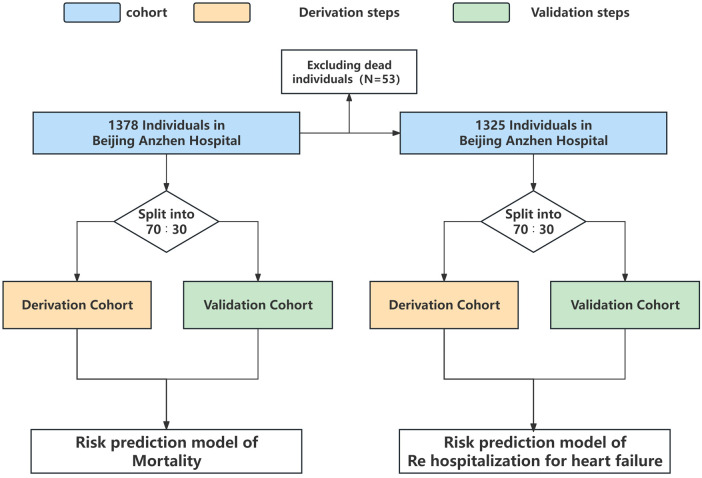
Personalized risk prediction system of mortality and rehospitalization for heart failure was developed. For developing a prediction system with death as the outcome, there were 965 patients (70%) and 413 patients (30%) were included in the the derivation cohort and the validation cohort. For developing a prediction system with rehospitalization for heart failure as the outcome, there were 927 patients (70%) and 398 patients (30%) were included in the derivation cohort and the validation cohort. There were 42 routine clinical variables used to develop the models. The performance evaluation of the model is based on the area under the curve (AUC). Evaluate the improvement with Euro Score II according to NRI and IDI net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
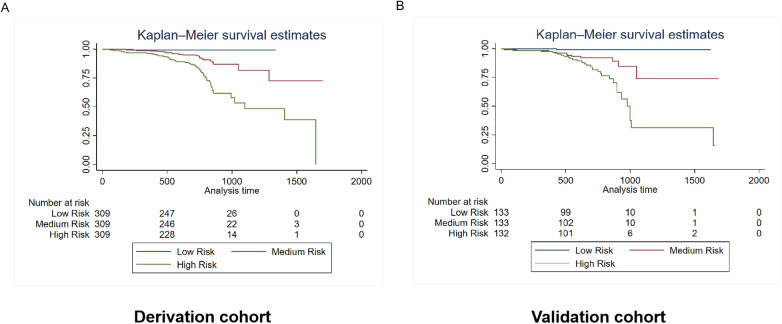
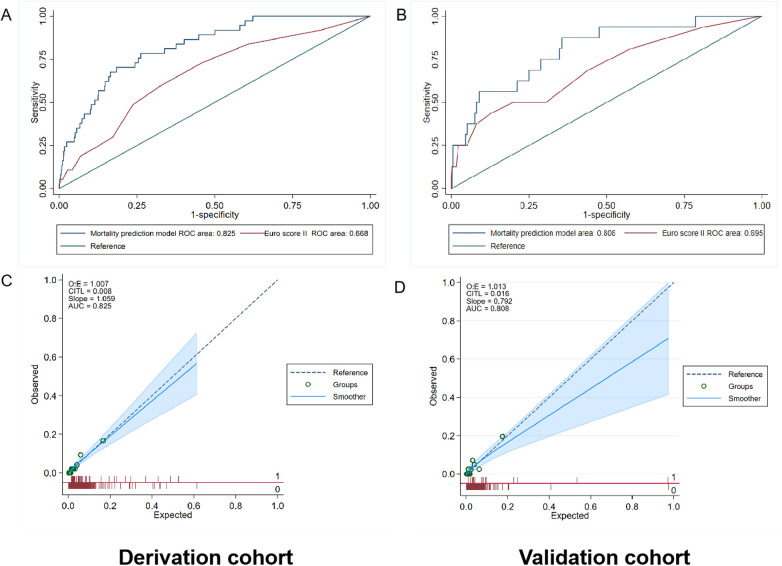
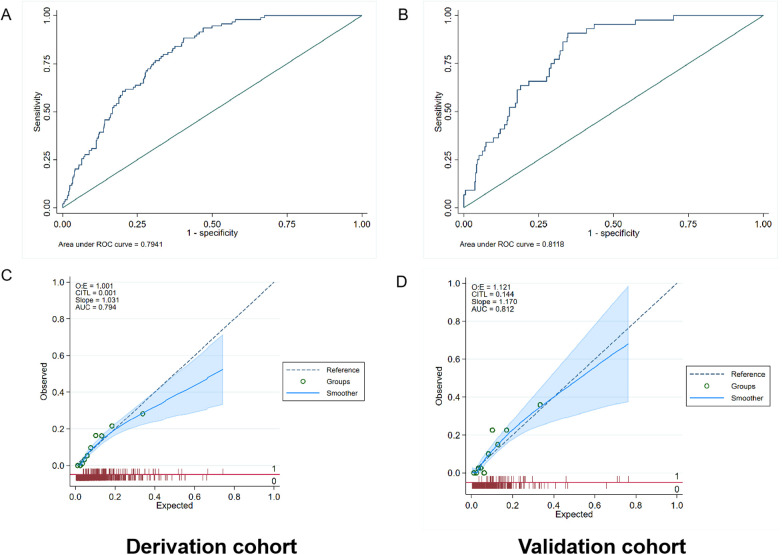
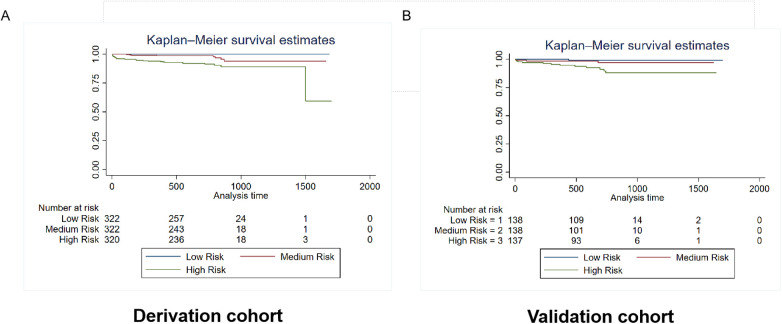
The median follow-up time was 685 days, the incidence of death was 3.85% ( = 53), and the incidence of rehospitalization for heart failure was 10.01% ( = 138). The AUC values of the mortality prediction model in the derivation and validation cohorts were 0.825 (0.764-0.886) and 0.808 (0.699-0.917), respectively. The AUC values of the rehospitalization for heart failure prediction model in the derivation and validation cohorts were 0.794 (0.756-0.832) and 0.812 (0.758-0.866), respectively. NRI and IDI showed that the mortality prediction model exhibited superior performance than the Euro Score II. The mortality and rehospitalization for heart failure risk prediction models effectively stratified patients into different risk subgroups.
The developed and validated models exhibit satisfactory performance in prediction of all-cause mortality and rehospitalization for heart failure after mitral valve repair surgery.
http://www.clinicaltrials.gov, Unique identifier: (NCT05141292).
准确评估二尖瓣修复手术患者术后的死亡率和心力衰竭再住院风险对于个体化医疗策略至关重要。
我们试图开发并验证一种用于预测死亡率和心力衰竭再住院的风险评估系统。
开发了心力衰竭死亡率和再住院的个性化风险预测系统。为开发以死亡为结局的预测系统,推导队列纳入965例患者(70%),验证队列纳入413例患者(30%)。为开发以心力衰竭再住院为结局的预测系统,推导队列纳入927例患者(70%),验证队列纳入398例患者(30%)。使用42个常规临床变量来构建模型。模型的性能评估基于曲线下面积(AUC)。根据净重新分类改善(NRI)和综合判别改善(IDI)评估与欧洲心脏手术风险评估系统II(Euro Score II)相比的改善情况。
中位随访时间为685天,死亡率为3.85%(n = 53),心力衰竭再住院率为10.01%(n = 138)。死亡率预测模型在推导队列和验证队列中的AUC值分别为0.825(0.764 - 0.886)和0.808(0.699 - 0.917)。心力衰竭再住院预测模型在推导队列和验证队列中的AUC值分别为0.794(0.756 - 0.832)和0.812(0.758 - 0.866)。NRI和IDI表明死亡率预测模型表现优于欧洲心脏手术风险评估系统II。死亡率和心力衰竭再住院风险预测模型有效地将患者分层到不同风险亚组。
所开发并验证的模型在预测二尖瓣修复手术后的全因死亡率和心力衰竭再住院方面表现出令人满意的性能。