Department of Community Medicine and School of Public Health, Postgraduate Institute of Medical Education and Research, Sector 12, Chandigarh, 160012, India.
Center for Community Medicine, All India Institute of Medical Sciences, New Delhi, 110049, India.
Sci Rep. 2024 Nov 19;14(1):28597. doi: 10.1038/s41598-024-80346-w.
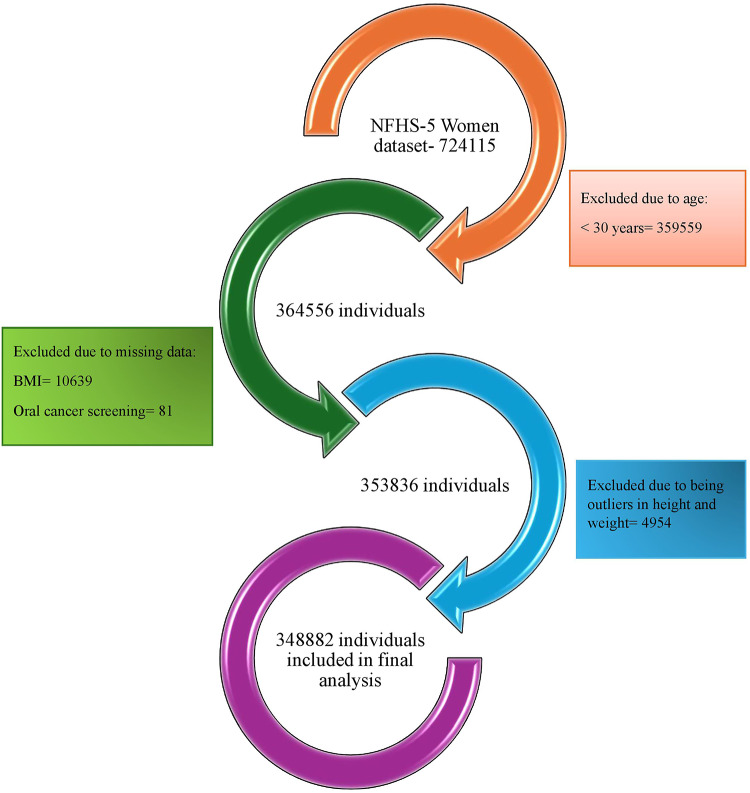
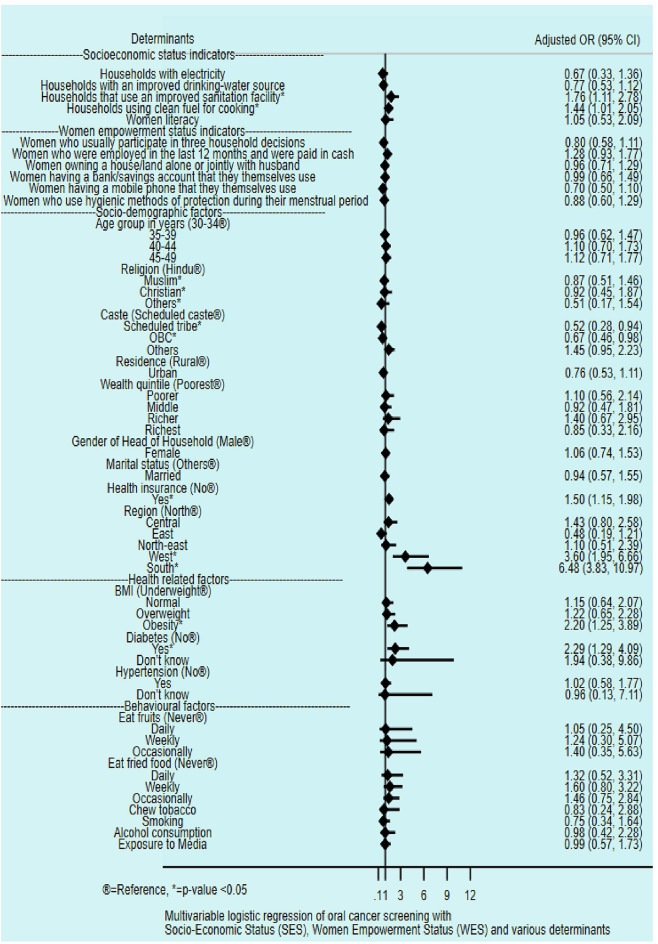
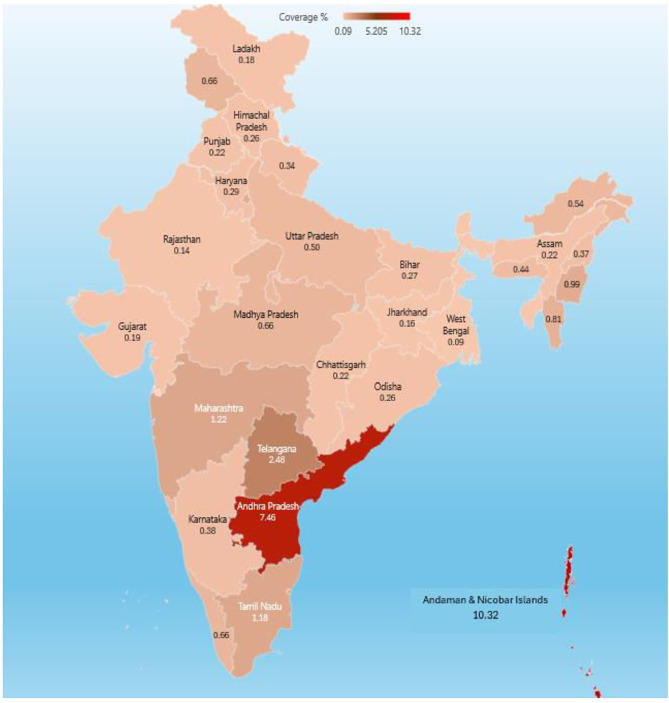
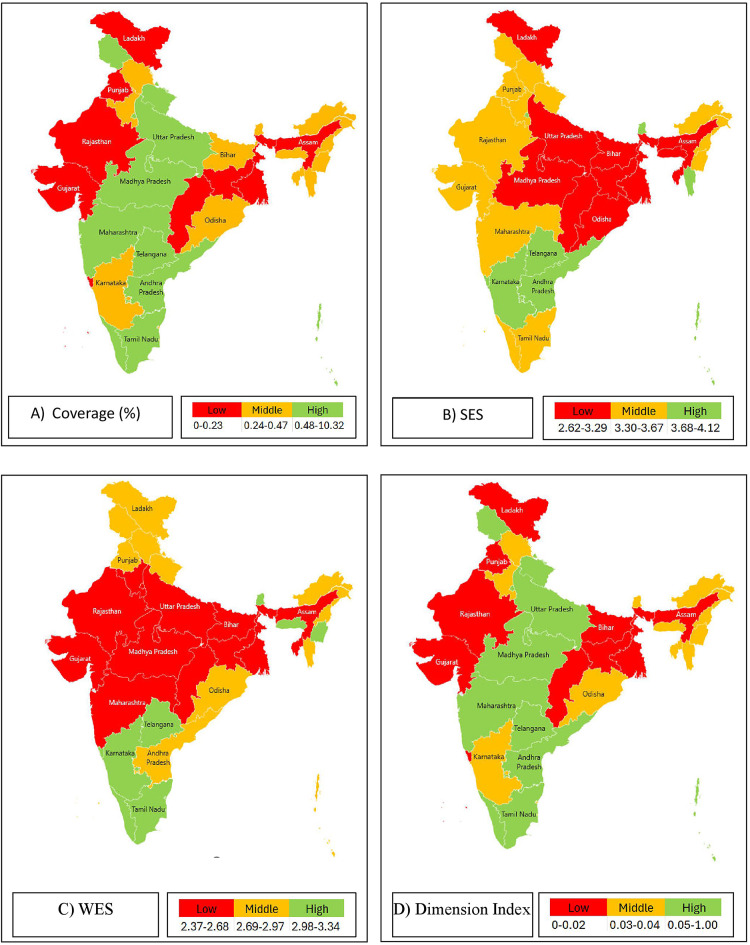
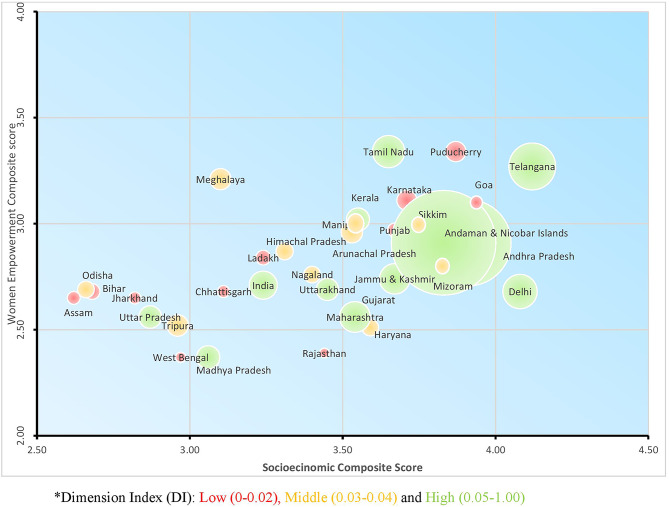
Oral cancer is the second most prevalent cancer in India and 5% of all cancers in women is contributed by oral cancer. In spite of being a part of national programme, the screening coverage rates remain low. Studies have indicated that the societal status of women and their empowerment plays a role in screening coverage for cancer. The objective of the current study is to estimate the coverage of oral cancer screening among Indian women within reproductive age-group across Indian states and union territories (UTs), to explore the relationship of socioeconomic status (SES) and women empower status (WES) with oral cancer screening coverage across Indian states and union territories (UT). Data from the fifth round of the nationally representative cross-sectional survey (National Family Health Survey, NFHS-2019-2021) was used in the present study with 3,48,882 individuals being included in the final analysis. We have cross-tabulated SES and WES composite scores with the Dimension Index (DI) of screening and categorised states and UTs into low, middle and high. We have represented these values over the Indian map. The interaction among these was graphically represented by a bubble plot. Further, we estimated the association of each indicator of SES and WES with screening coverage using multivariable logistic regression. The national coverage of oral cancer screening among women of reproductive age was 0.77% with Andhra Pradesh (7%) and Andaman and Nicobar Islands (10%) recording the highest screening coverage. Despite having high SES and WES scores, Madhya Pradesh and Uttar Pradesh, the screening (DI) was low. States with both high women empowerment status and high socioeconomic status showed high oral cancer screening uptake but the trend was not universal. Still, there were variations in the association among the states. The increased screening was significantly associated with higher access to improved sanitary facility (76%) and clean fuel for cooking (44%). Socio-economic status is an important precursor for better oral cancer screening coverage but women empowerment status did not always translate into good cancer screening uptake. Deep-rooted socio-cultural constructs and stigma associated with cancer and its implications may play a role. Implementation research for better uptake of oral cancer screening coverage is required.
口腔癌是印度第二大常见癌症,女性癌症患者中有 5%是口腔癌。尽管口腔癌筛查已纳入国家项目,但筛查覆盖率仍然较低。研究表明,女性的社会地位和赋权对癌症筛查覆盖率起着一定的作用。本研究的目的是估计印度各邦和联邦属地(UT)中育龄期女性口腔癌筛查的覆盖情况,探索社会经济地位(SES)和妇女赋权地位(WES)与印度各邦和联邦属地(UT)口腔癌筛查覆盖之间的关系。本研究使用了具有全国代表性的横断面调查(国家家庭健康调查,NFHS-2019-2021)的第五轮数据,最终分析纳入了 348882 人。我们将 SES 和 WES 综合评分与筛查的维度指数(DI)进行交叉制表,并将邦和 UTs 分为低、中、高三种。我们在印度地图上表示了这些值。这些值之间的相互作用通过气泡图进行了图形表示。此外,我们使用多变量逻辑回归估计了 SES 和 WES 的每个指标与筛查覆盖率的关联。在育龄妇女中,口腔癌筛查的全国覆盖率为 0.77%,其中安得拉邦(7%)和安达曼和尼科巴群岛(10%)的筛查覆盖率最高。尽管孟买和北方邦的 SES 和 WES 得分较高,但筛查(DI)却较低。妇女赋权地位和社会经济地位均较高的邦,口腔癌筛查的参与度较高,但这种趋势并非普遍存在。尽管如此,各州之间的关联仍存在差异。筛查率的提高与更好地获得改良卫生设施(76%)和清洁烹饪燃料(44%)显著相关。社会经济地位是提高口腔癌筛查覆盖率的重要前提,但妇女赋权地位并不总是转化为良好的癌症筛查参与度。与癌症及其影响相关的根深蒂固的社会文化观念和耻辱感可能会起到一定的作用。需要进行实施研究,以提高口腔癌筛查的覆盖率。