Department of Psychology, University of Bath, Bath, BA2 7AY, UK.
Division of Psychology and Mental Health, School of Health Sciences, University of Manchester, Manchester, UK.
BMC Psychiatry. 2024 Nov 19;24(1):821. doi: 10.1186/s12888-024-06294-x.
Consensus on what outcomes should be included in trials of psychological therapies on acute psychiatric inpatient wards is currently lacking. Inclusion of different viewpoints, including service user perspectives, is crucial in ensuring that future trials measure outcomes which are meaningful and important. Development of a Core Outcome Set (COS), a minimum standardised set of outcomes to be measured and reported, would help improve synthesis and interpretation of clinical trial data in this area.
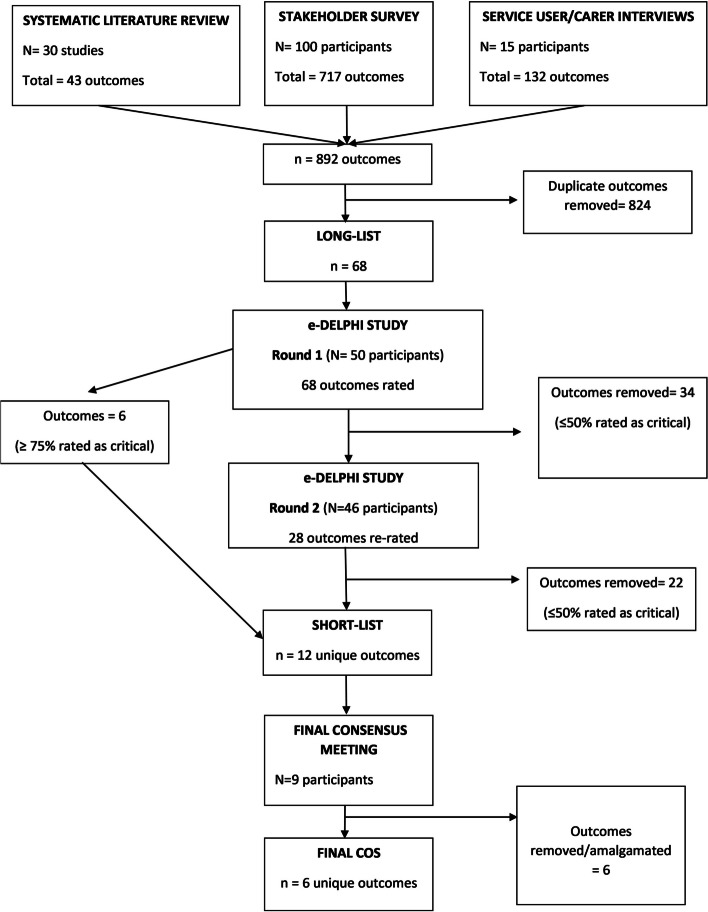
Stage 1 of the COS development involved compiling a comprehensive long-list of outcomes from key sources including i) a systematic review of outcomes from published trials, ii) online survey of key stakeholders (service users, carers, healthcare professionals, researchers, and end users of research), iii) qualitative interviews with service users and carers. Stage 2 involved stakeholder groups short-listing the outcomes using consensus methods (e-Delphi survey). The final outcome set was derived from the short-list at a consensus meeting of stakeholders, facilitated by an Independent Chair.
A long-list of 68 outcomes was compiled from the systematic review (n = 30 trials), online stakeholder survey (n = 100 participants) and qualitative interviews (n = 15 participants). Fifty stakeholders took part in the e-Delphi study, where the long-list was cut down to a short-list of 12 outcomes over 2 rounds. Nine stakeholders took part in the final consensus meeting, and after some outcomes were removed and/or amalgamated, a final set of 6 outcomes was recommended for inclusion in the COS. These were Ability to Cope, Hopefulness, Quality of Life, Psychosis Symptoms, Mood, and Self-Harm Behaviours.
Widespread future adoption of the COS will reduce research waste by ensuring that outcomes are more easily comparable across trials, and that the full range of stakeholder priorities are represented in trial outcomes. This makes it more likely that effective therapies will be identified in a timely fashion and successfully implemented in routine clinical practice. The final 6-outcome COS should be feasible to implement given the need keep participant burden to a minimum in inpatient trials. Further work is needed to make recommendations for the best outcome measurement instruments to use, including the use of patient-reported outcomes alongside clinician-rated measures.
Not applicable.
目前,对于急性精神病住院病房心理治疗试验应纳入哪些结局,尚未达成共识。纳入不同观点,包括服务使用者的观点,对于确保未来的试验能够测量有意义和重要的结局至关重要。制定核心结局集(COS),即一套标准化的最小结局测量和报告集,将有助于改善该领域临床试验数据的综合和解释。
COS 开发的第一阶段涉及从关键来源(包括 i)系统综述已发表试验的结局、ii)在线调查关键利益相关者(服务使用者、照顾者、医疗保健专业人员、研究人员和研究成果的最终使用者)、iii)与服务使用者和照顾者的定性访谈)中编制一份全面的长列表结局。第二阶段涉及利益相关者使用共识方法(电子德尔菲调查)对结局进行短名单筛选。最终的结局集源自利益相关者共识会议上的短名单,由独立主席协助。
从系统综述(n=30 项试验)、在线利益相关者调查(n=100 名参与者)和定性访谈(n=15 名参与者)中编制了一份 68 项结局的长列表。50 名利益相关者参与了电子德尔菲研究,在两轮中,长列表被缩减为 12 项的短列表。9 名利益相关者参加了最终的共识会议,在删除和/或合并了一些结局后,推荐了 6 项最终结局纳入 COS。这些结局包括应对能力、希望、生活质量、精神病症状、情绪和自伤行为。
广泛采用 COS 将通过确保试验之间的结局更易于比较,并代表利益相关者的全部优先事项,来减少研究浪费。这使得更有可能及时发现有效的治疗方法,并成功将其应用于常规临床实践。鉴于需要将参与者的负担降到最低,最终的 6 项结局 COS 应该是可行的。需要进一步的工作来制定使用最佳结局测量工具的建议,包括使用患者报告结局和临床医生评定的测量方法。
不适用。