Kumagai Naonori, Takao Hiroki, Sudo Yuta, Yoshikane Masatoshi, Kondoh Tomomi, Matsumoto Yuji, Mizuno Haruo, Abe Michiaki, Ikezumi Yohei
Department of Pediatrics, Fujita Health University School of Medicine, Toyoake, Japan.
Department of Education and Support for Regional Medicine, Tohoku University Hospital, Sendai, Japan.
Diabetol Metab Syndr. 2024 Nov 20;16(1):276. doi: 10.1186/s13098-024-01506-6.
Proximal renal tubular dysfunction occurs during diabetic ketoacidosis (DKA) in type 1 diabetes. However, only a few studies have reported on the multiple proximal renal tubular functions simultaneously. Moreover, to the best of our knowledge, distal renal tubular function has not yet been investigated.
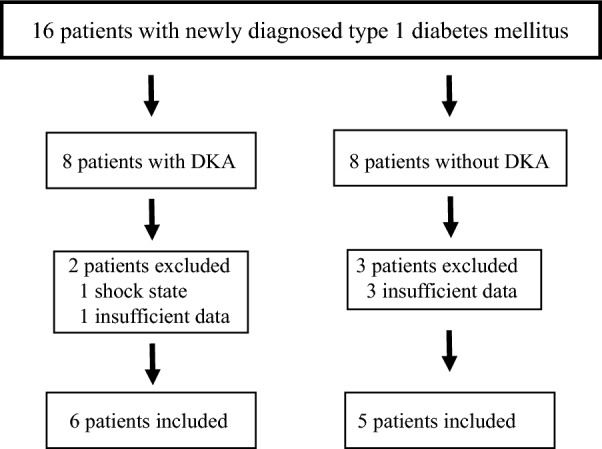
Patients with newly diagnosed type 1 diabetes mellitus were classified into those with DKA and those without DKA, and their proximal and distal renal tubular functions were investigated. The diagnostic criteria for DKA were blood glucose > 200 mg/dL, blood pH < 7.3 or HCO < 15 mEq/L, and urine ketone body positivity.
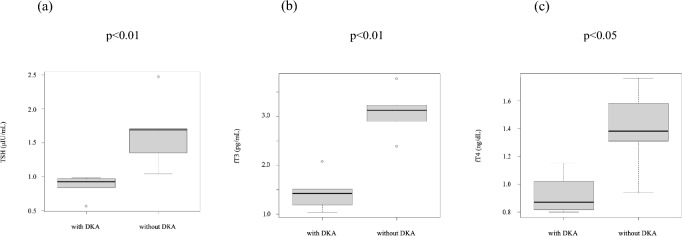
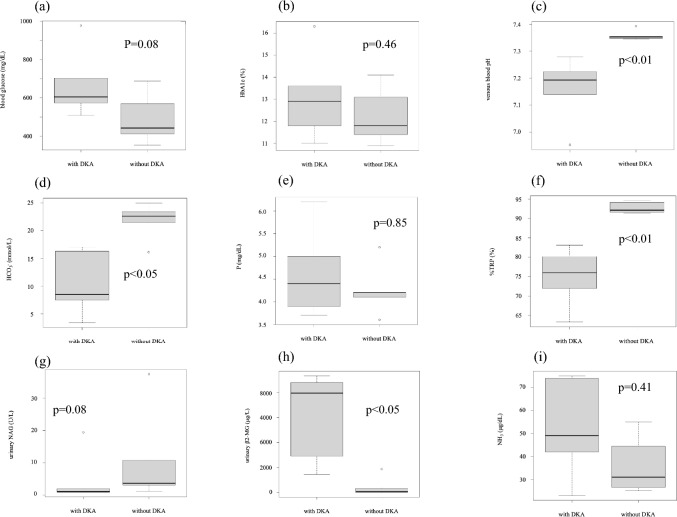
Six patients with DKA and five patients without DKA were included. In patients with DKA, urinary β2-microglobulin levels were significantly higher, while blood pH, HCO, and tubular reabsorption of phosphorus were significantly lower than in those without DKA. There were no significant differences in blood glucose, HbA1c, serum phosphorus, urinary N-acetyl-beta-glucosaminidase, and urinary amino acid excretion between patients with and without DKA. Elevated NH levels and impaired urinary acidification were not observed in patients with and without DKA.
In patients with newly diagnosed type 1 diabetes mellitus complicated with DKA, multiple proximal renal tubular dysfunctions occur simultaneously, suggesting transient Fanconi syndrome. Distal renal tubular acidosis was unlikely. The diagnostic criteria for DKA are appropriate also in the view of proximal renal tubular dysfunction and are considered suggestive of pathophysiological factors that may cause proximal renal tubular dysfunction.
1型糖尿病患者在糖尿病酮症酸中毒(DKA)期间会出现近端肾小管功能障碍。然而,仅有少数研究同时报道了多种近端肾小管功能。此外,据我们所知,尚未对远端肾小管功能进行研究。
将新诊断的1型糖尿病患者分为发生DKA组和未发生DKA组,并对其近端和远端肾小管功能进行研究。DKA的诊断标准为血糖>200mg/dL、血pH<7.3或HCO<15mEq/L以及尿酮体阳性。
纳入6例发生DKA的患者和5例未发生DKA的患者。发生DKA的患者尿β2-微球蛋白水平显著升高,而血pH、HCO以及磷的肾小管重吸收显著低于未发生DKA的患者。发生DKA和未发生DKA的患者在血糖、糖化血红蛋白、血清磷、尿N-乙酰-β-氨基葡萄糖苷酶以及尿氨基酸排泄方面无显著差异。发生DKA和未发生DKA的患者均未观察到NH水平升高和尿酸化受损。
新诊断的1型糖尿病合并DKA的患者会同时出现多种近端肾小管功能障碍,提示为暂时性范科尼综合征。远端肾小管酸中毒不太可能。从近端肾小管功能障碍的角度来看,DKA的诊断标准也是合适的,并且被认为提示了可能导致近端肾小管功能障碍的病理生理因素。