Wang Michael Ke, Devereaux P J, Marcucci Maura, Lomivorotov Vladimir, Sessler Daniel I, Chan Matthew T V, Borges Flavia K, Ofori Sandra N, Paniagua Pilar, Douketis James D, Sigamani Alben, Parlow Joel L, Wang Chew Y, Villar Juan Carlos, Srinathan Sadeesh K, Szczeklik Wojciech, Martínez-Zapata María José, Malaga German, Sivakumaran Soori, McIntyre William F, Rodríguez Funes María-Virginia, Cruz Patricia, Alvarez-Garcia Jesús, Greiss Isabelle, Popova Ekaterine, Hemels Martin E, Brandes Axel, Chow Clara K, Barnawal Satish Prasad, Healey Jeff S, Conen David
Department of Medicine, McMaster University, Hamilton, Ontario, Canada.
Population Health Research Institute, McMaster University, Hamilton, Ontario, Canada.
CJC Open. 2024 Aug 17;6(11):1363-1371. doi: 10.1016/j.cjco.2024.08.003. eCollection 2024 Nov.
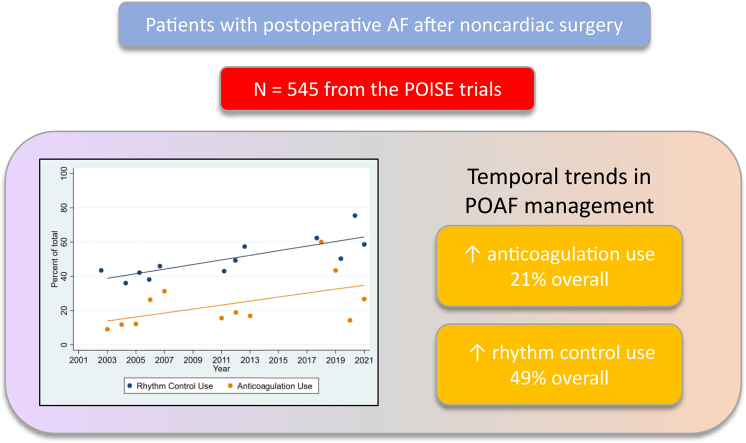
Clinically important perioperative atrial fibrillation (POAF) is a common cardiac complication after noncardiac surgery. Little is known about how patients with POAF are managed acutely and whether practices have changed over time.
We conducted an observational substudy of patients who had POAF, were at elevated cardiovascular risk, and were enrolled in the PeriOperative Ischemic Evaluation (POISE)-1, 2 and 3 trials between 2002 and 2021. POAF was defined as new, clinically important atrial fibrillation occurring within 30 days after surgery. We assessed the use of rhythm-control and anticoagulation treatment in response to POAF, at hospital discharge and at 30 days after surgery. We assessed for temporal trends using multivariable logistic regression.
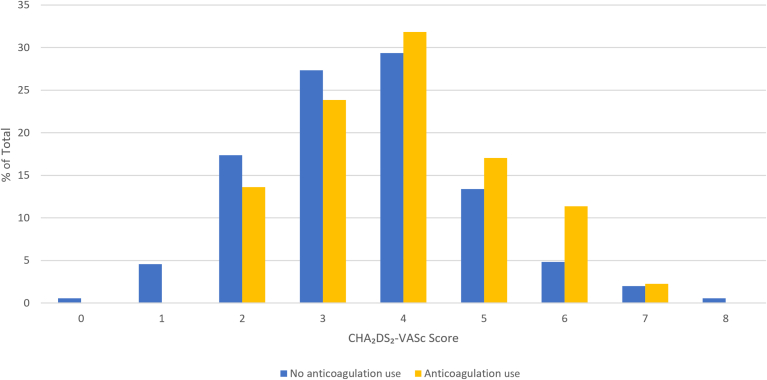
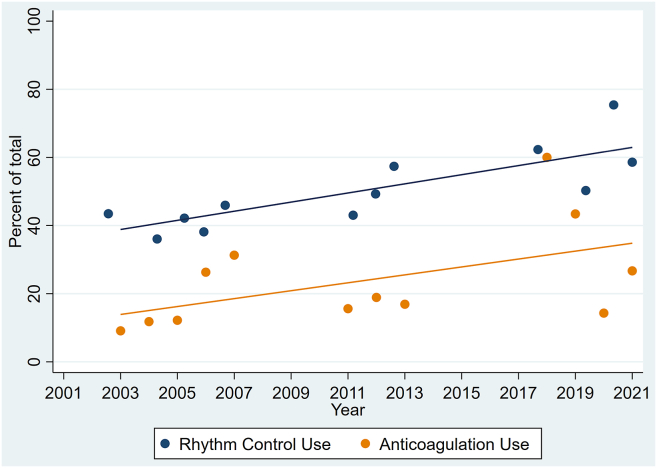
Of the 27,896 patients included, 545 (1.9%) developed clinically important POAF. Patients received rhythm-control treatment in 48.6% of cases. The level of use of rhythm-control treatment increased over the course of the trials (POISE-1 vs POISE-2 vs POISE-3; 40.9% vs 49.5% vs 59.1%). A later randomization date was associated independently with use of rhythm-control treatment (odds ratio, 1.05 per year; 95% confidence interval, 1.01-1.09). Anticoagulation treatment was prescribed in 21% of POAF cases. The level of anticoagulation treatement use was higher in POISE-3, compared to that in the 2 previous trials (POISE-1 vs POISE-2 vs POISE-3-16.4% vs 16.5% vs 33.6%). A later randomization date was associated independently with use of anticoagulation treatment (odds ratio, 1.06 per year; 95% confidence interval, 1.02-1.11).
Despite the absence of randomized controlled trials, the level of use of rhythm-control and anticoagulation treatment for POAF is rising. High-quality trials are needed urgently to determine whether these interventions are safe and effective in this population.
具有临床意义的围手术期房颤(POAF)是心脏手术以外的其他手术常见的心脏并发症。对于POAF患者如何进行急性处理以及相关做法是否随时间发生了变化,人们了解甚少。
我们对患有POAF、心血管风险升高且在2002年至2021年期间参加围手术期缺血评估(POISE)-1、2和3试验的患者进行了一项观察性子研究。POAF定义为术后30天内出现的新的、具有临床意义的房颤。我们评估了出院时和术后30天时针对POAF使用节律控制和抗凝治疗的情况。我们使用多变量逻辑回归评估时间趋势。
在纳入的27,896例患者中,545例(1.9%)发生了具有临床意义的POAF。48.6%的病例接受了节律控制治疗。在试验过程中,节律控制治疗的使用水平有所提高(POISE-1对比POISE-2对比POISE-3;40.9%对比49.5%对比59.1%)。随机分组日期越晚,与使用节律控制治疗独立相关(比值比,每年1.05;95%置信区间,1.01-1.09)。21%的POAF病例接受了抗凝治疗。与前两项试验相比,POISE-3中抗凝治疗的使用水平更高(POISE-1对比POISE-2对比POISE-3-16.4%对比16.5%对比33.6%)。随机分组日期越晚,与使用抗凝治疗独立相关(比值比,每年1.06;95%置信区间,1.02-1.11)。
尽管缺乏随机对照试验,但针对POAF的节律控制和抗凝治疗的使用水平正在上升。迫切需要高质量的试验来确定这些干预措施在该人群中是否安全有效。