National Center for Collaborative Healthcare Innovation, Veterans Affairs Palo Alto Health Care System, Palo Alto, CA, United States.
JMIR Nurs. 2024 Nov 22;7:e59619. doi: 10.2196/59619.
Optimal nurse staffing levels have been shown to impact patients' prognoses and safety, as well as staff burnout. The predominant method for calculating staffing levels has been patient-to-nurse (P/N) ratios and nursing hours per patient day. However, both methods fall short of addressing the dynamic nature of staffing needs that often fluctuate throughout the day as patients' clinical status changes and new patients are admitted or discharged from the unit.
In this evaluation, the Veterans Affairs Palo Alto Health Care System (VAPAHCS) piloted a new dynamic bed count calculation in an effort to target optimal staffing levels every hour to provide greater temporal resolution on nurse staffing levels within the Veterans Health Administration.
The dynamic bed count uses elements from both the nursing hours per patient day and P/N ratio to calculate current and target staffing levels, every hour, while balancing across nurse types (registered nurses to nurse assistants) to provide improved temporal insight into staff allocation. The dynamic bed count was compared with traditional P/N ratio methods of calculating patient capacity at the VAPAHCS, to assess optimal patient capacity within their acute care ward from January 1, 2023, through May 25, 2023. Descriptive statistics summarized patient capacity variables across the intensive care unit (ICU), medical-surgical ICU, and 3 acute care units. Student t tests (2-tailed) were used to analyze differences between patient capacity measures.
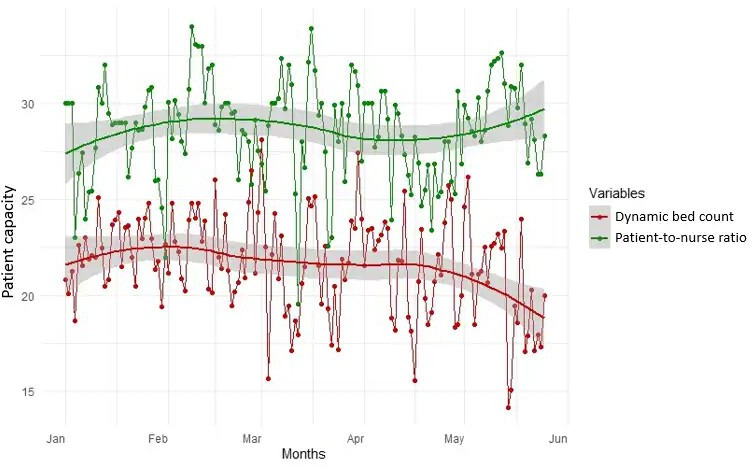
Hourly analysis of patient capacity information displayed how the dynamic bed count provided improved temporal resolution on patient capacity. Comparing the dynamic bed count to the P/N ratio, we found the patient capacity, as determined by the P/N ratio, was, on average, higher than that of the dynamic bed count across VAPAHCS acute care units and the medical-surgical ICU (P<.001). For example, in acute care unit 3C, the average dynamic bed count was 21.6 (SD 4.2) compared with a P/N ratio of 28.6 (SD 3.2). This suggests that calculating patient capacity using P/N ratios alone could lead to units taking on more patients than what the dynamic bed count suggests the unit can optimally handle.
As a new patient capacity calculation, the dynamic bed count provided additional details and timely information about clinical staffing levels, patient acuity, and patient turnover. Implementing this calculation into the management process has the potential to empower departments to further optimize staffing and patient care.
已证实,最佳护士配备水平会影响患者的预后和安全,以及员工的倦怠程度。计算人员配备水平的主要方法是患者与护士的比例(P/N 比)和每位患者每天的护理小时数。然而,这两种方法都未能解决人员配备需求的动态性质,因为随着患者临床状况的变化以及新患者入院或出院,人员配备需求在一天中经常波动。
在这项评估中,退伍军人事务帕洛阿尔托医疗保健系统(VAPAHCS)试点了一种新的动态床位计算方法,旨在每小时确定最佳人员配备水平,以便在退伍军人健康管理局内提供更具时间分辨率的护士人员配备水平。
动态床位计数使用患者每天护理小时数和 P/N 比中的元素来计算当前和目标人员配备水平,每小时一次,同时平衡护士类型(注册护士到护士助理)以提供对员工分配的更深入的时间洞察力。动态床位计数与 VAPAHCS 计算患者容量的传统 P/N 比方法进行了比较,以评估急性护理病房内的最佳患者容量,时间范围为 2023 年 1 月 1 日至 2023 年 5 月 25 日。描述性统计数据总结了重症监护病房(ICU)、内科-外科 ICU 和 3 个急性护理病房的患者容量变量。使用学生 t 检验(双侧)分析患者容量测量值之间的差异。
患者容量信息的每小时分析显示了动态床位计数如何提供对患者容量的更具时间分辨率的了解。将动态床位计数与 P/N 比进行比较,我们发现,根据 P/N 比确定的患者容量在 VAPAHCS 急性护理病房和内科-外科 ICU 中平均高于动态床位计数(P<.001)。例如,在 3C 急性护理病房,平均动态床位计数为 21.6(SD 4.2),而 P/N 比为 28.6(SD 3.2)。这表明,仅使用 P/N 比计算患者容量可能导致单位承担比动态床位计数建议的单位能够最佳处理的更多患者。
作为一种新的患者容量计算方法,动态床位计数提供了有关临床人员配备水平、患者病情严重程度和患者周转率的更多详细信息和及时信息。将此计算纳入管理流程有可能使部门能够进一步优化人员配备和患者护理。