Department of Renal Medicine, Aarhus University Hospital, Aarhus, 8200, Denmark.
Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark.
BMC Nephrol. 2024 Nov 27;25(1):426. doi: 10.1186/s12882-024-03876-5.
Patients with chronic kidney disease (CKD) are susceptible to vascular calcification and vitamin K deficiency. Matrix gla protein (MGP) is a potent inhibitor of calcification requiring vitamin K for activation. Inactive MGP, i.e. dephosphorylated uncarboxylated MGP (dp-ucMGP), is frequently elevated in CKD along with protein induced by vitamin K absence (PIVKA-II). We investigated whether dp-ucMGP and PIVKA-II are useful markers of aortic calcification in CKD.
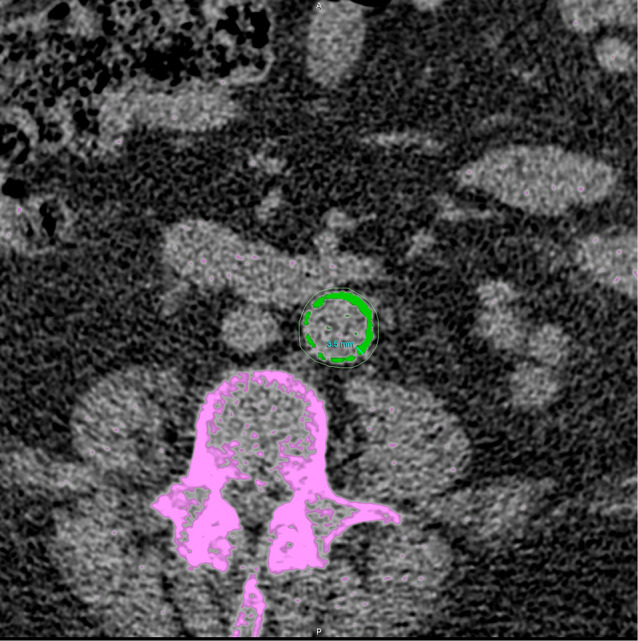
Patients with normal or reduced kidney function underwent a non-contrast computed tomography scan of the entire aorta with subsequent blinded standard calcification scoring of the aortic wall ad modum Agatston. Blood samples were analyzed for plasma concentrations of dp-ucMGP and PIVKA-II.
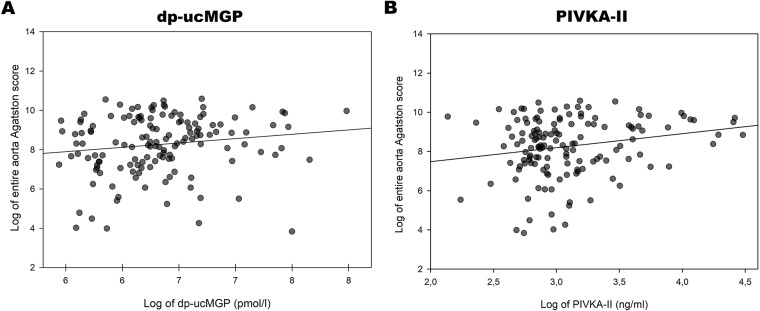
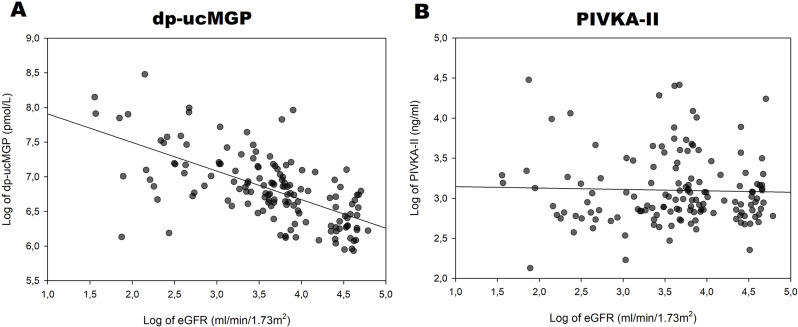
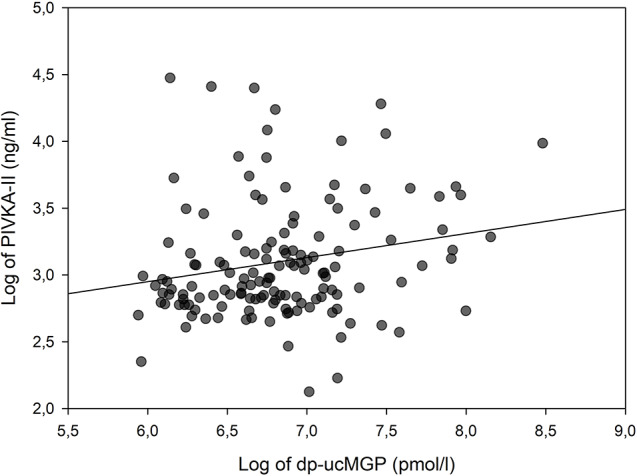
141 patients (104 with CKD stage 3-5) were included. In patients with/without CKD median (interquartile range) were dp-ucMGP 543 (503-744)/1078 (835-1682) pmol/l (P < 0.01); PIVKA-II 19.3 (16.3-23.5)/21.8 (17.2-36.8) ng/ml (P = 0.33) and aortic Agatston scores 1644 (729-4138)/7172 (2834-15360) (P < 0.01). Agatston score was positively associated with PIVKA-II (β = 0.71, P = 0.014, r = 0.04) and tended to be so with dp-ucMGP (β = 0.44, P = 0.08, r = 0.02). Age, estimated glomerular filtration rate (eGFR) and smoking status were also associated with Agatston score and remained so, along with PIVKA-II, when adjusted for potential confounders. However, the association between age and aortic Agatston score was stronger than for PIVKA-II, eGFR and smoking-status.
Vitamin K deficiency, as estimated through PIVKA-II, but not dp-ucMGP, is weakly associated with aortic Agatston score. Yet, as markers of aortic calcification, both were outperformed substantially by age, and neither surpassed smoking nor eGFR.
NCT04114695.
慢性肾脏病(CKD)患者易发生血管钙化和维生素 K 缺乏。基质 Gla 蛋白(MGP)是一种有效的钙化抑制剂,需要维生素 K 激活。无活性的 MGP,即去磷酸化未羧化 MGP(dp-ucMGP),在 CKD 中常与维生素 K 缺乏诱导蛋白(PIVKA-II)一起升高。我们研究了 dp-ucMGP 和 PIVKA-II 是否可作为 CKD 主动脉钙化的有用标志物。
肾功能正常或降低的患者进行了整个主动脉的非对比计算机断层扫描,随后对主动脉壁进行盲法标准钙化评分,采用 Agatston 评分法。分析血样中 dp-ucMGP 和 PIVKA-II 的血浆浓度。
共纳入 141 例患者(104 例 CKD 3-5 期)。CKD 患者和非 CKD 患者的 dp-ucMGP 中位数(四分位距)分别为 543(503-744)/1078(835-1682)pmol/L(P<0.01);PIVKA-II 中位数(四分位距)分别为 19.3(16.3-23.5)/21.8(17.2-36.8)ng/ml(P=0.33);主动脉 Agatston 评分中位数(四分位距)分别为 1644(729-4138)/7172(2834-15360)(P<0.01)。Agatston 评分与 PIVKA-II 呈正相关(β=0.71,P=0.014,r=0.04),与 dp-ucMGP 呈弱相关趋势(β=0.44,P=0.08,r=0.02)。年龄、估算肾小球滤过率(eGFR)和吸烟状态也与 Agatston 评分相关,在调整了潜在混杂因素后,仍与 PIVKA-II 相关。然而,年龄与主动脉 Agatston 评分的相关性强于 PIVKA-II、eGFR 和吸烟状况。
通过 PIVKA-II 估计的维生素 K 缺乏与主动脉 Agatston 评分呈弱相关,而非 dp-ucMGP。然而,作为主动脉钙化的标志物,二者均明显逊于年龄,且均不如吸烟或 eGFR 。
NCT04114695