Krittanawong Chayakrit, Castillo Rodriguez Beatriz, Ang Song Peng, Qadeer Yusuf Kamran, Wang Zhen, Alam Mahboob, Sharma Samin, Jneid Hani
Cardiology Division, NYU Langone Health and NYU School of Medicine, New York, NY 10016, USA.
Division of Internal Medicine, Baylor College of Medicine, Houston, TX 77030, USA.
Rev Cardiovasc Med. 2024 Nov 18;25(11):404. doi: 10.31083/j.rcm2511404. eCollection 2024 Nov.
Spontaneous coronary artery dissection (SCAD) is a rare and often underdiagnosed cause of acute coronary syndrome (ACS), predominantly affecting younger women without traditional cardiovascular risk factors. The management of SCAD remains a subject of debate, likely secondary to inconclusive evidence. This study aims to compare the clinical outcomes of SCAD patients treated with optimal medical therapy (OMT) versus those who underwent percutaneous coronary intervention (PCI) using a national population-based cohort.
We conducted a retrospective analysis using the National Inpatient Sample (NIS) database from 2016 to 2020. The study included patients identified with SCAD using the ICD-10-CM (the International Classification of Diseases, Tenth Revision, Clinical Modification) code I25.42. We excluded individuals who did not receive PCI or coronary angiography, those who underwent coronary artery bypass grafting, and patients with incomplete records. The primary outcome was in-hospital mortality, while secondary outcomes included acute kidney injury, cardiac arrest, cardiogenic shock, use of temporary mechanical circulatory support, cost of hospitalization, and length of stay. National estimates were obtained using discharge weights, and statistical comparisons were performed using chi-square tests and linear regression. Multivariate logistic regression was employed to identify predictors of mortality and other outcomes.
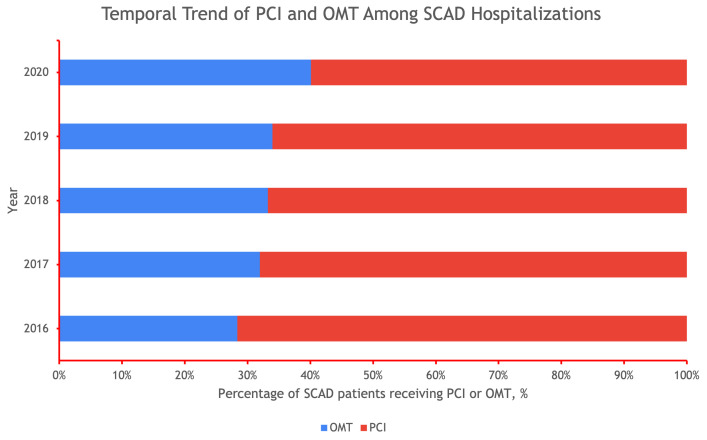
A total of 31,105 SCAD patients were included in the study, with 10,480 receiving OMT and 20,625 undergoing PCI. Patients in the PCI group were older (mean age 64 vs. 54 years) and had higher comorbidities compared to those in the OMT group. The proportion of SCAD patients receiving PCI declined from 72% in 2016 to 60% in 2020. In multivariable analysis, PCI was associated with increased in-hospital mortality (odds ratio (OR) 1.89, 95% confidence interval (CI) 1.24-2.90, = 0.0003), cardiogenic shock (OR 2.29, 95% CI 1.71-3.07, < 0.0001), use of a left ventricular assist device (LVAD) (OR 3.97, 95% CI 2.42-6.53, < 0.0001), and an intra-aortic balloon pump (IABP) (OR 2.24, 95% CI 1.63-3.09, < 0.0001). Trends also suggested an association between PCI and cardiac arrest, extracorporeal membrane oxygenation (ECMO), and acute kidney injury (AKI). The PCI group had significantly higher hospitalization costs and longer lengths of stay compared to the OMT group (both < 0.001).
In this large, national cohort study, SCAD patients who underwent PCI had significantly higher risks of adverse in-hospital outcomes, including mortality, compared to those treated with OMT. These findings underscore the importance of careful patient selection and the potential advantages of conservative management in SCAD, particularly in patients without severe or unstable presentations. Further research is needed to develop evidence-based guidelines for the optimal management of SCAD.
自发性冠状动脉夹层(SCAD)是急性冠状动脉综合征(ACS)的一种罕见且常被漏诊的病因,主要影响无传统心血管危险因素的年轻女性。SCAD的治疗仍是一个有争议的话题,可能是由于证据不确凿。本研究旨在使用全国性基于人群的队列,比较接受最佳药物治疗(OMT)的SCAD患者与接受经皮冠状动脉介入治疗(PCI)的患者的临床结局。
我们使用2016年至2020年的全国住院患者样本(NIS)数据库进行了一项回顾性分析。该研究纳入了使用ICD-10-CM(国际疾病分类第十次修订版临床修订本)编码I25.42确诊为SCAD的患者。我们排除了未接受PCI或冠状动脉造影的个体、接受冠状动脉旁路移植术的患者以及记录不完整的患者。主要结局是住院死亡率,次要结局包括急性肾损伤、心脏骤停、心源性休克、使用临时机械循环支持、住院费用和住院时间。使用出院权重获得全国估计值,并使用卡方检验和线性回归进行统计比较。采用多变量逻辑回归来确定死亡率和其他结局的预测因素。
本研究共纳入31105例SCAD患者,其中10480例接受OMT,20625例接受PCI。PCI组患者年龄较大(平均年龄64岁对54岁),与OMT组相比合并症更多。接受PCI的SCAD患者比例从2016年的72%下降到2020年的60%。在多变量分析中,PCI与住院死亡率增加相关(比值比(OR)1.89,95%置信区间(CI)1.24 - 2.90,P = 0.0003)、心源性休克(OR 2.29,95% CI 1.71 - 3.07,P < 0.0001)、使用左心室辅助装置(LVAD)(OR 3.97,95% CI 2.42 - 6.53,P < 0.0001)和主动脉内球囊泵(IABP)(OR 2.24,95% CI 1.63 - 3.09,P < 0.0001)相关。趋势也表明PCI与心脏骤停、体外膜肺氧合(ECMO)和急性肾损伤(AKI)之间存在关联。与OMT组相比,PCI组的住院费用显著更高,住院时间更长(均P < 0.001)。
在这项大型全国性队列研究中,与接受OMT治疗的SCAD患者相比,接受PCI治疗的患者发生包括死亡在内的不良住院结局的风险显著更高。这些发现强调了谨慎选择患者的重要性以及SCAD保守治疗的潜在优势,特别是在无严重或不稳定表现的患者中。需要进一步研究以制定基于证据的SCAD最佳管理指南。