Khanna Diana, Lay Kiri, Khadka Jyoti, Mpundu-Kaambwa Christine, Ratcliffe Julie
Health and Social Care Economics Group, Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, Adelaide, 5042, Australia.
Registry of Senior Australians, Healthy Ageing Research Consortium, South Australian Health and Medical Research Institute, Adelaide, Australia.
Health Qual Life Outcomes. 2024 Dec 5;22(1):105. doi: 10.1186/s12955-024-02320-4.
The EQ-5D-Y-3L is widely used for measuring and valuing HRQoL in paediatric populations. This mixed methods study used the EQ-5D-Y-3L measure and applied a retrospective think-aloud approach to examine the self-report validity in children of varying chronological age.
A mixed methods study was conducted in a community-based sample of 39 children aged 6-12 years. In a semi-structured interview, children self-completed the EQ-5D-Y-3L and then engaged in retrospective think-aloud. Conversations were audio-recorded and transcribed for analysis in NVivo using the Tourangeau four-stage response model framework to assess comprehension, judgment, recall, and response mapping issues. Fisher's exact test was used to assess the differences between child-self reported HRQoL across subgroups. The inter-rater agreement between child-parent dyads was assessed with CCC for overall HRQoL and Gwet's AC for dimension level HRQoL.
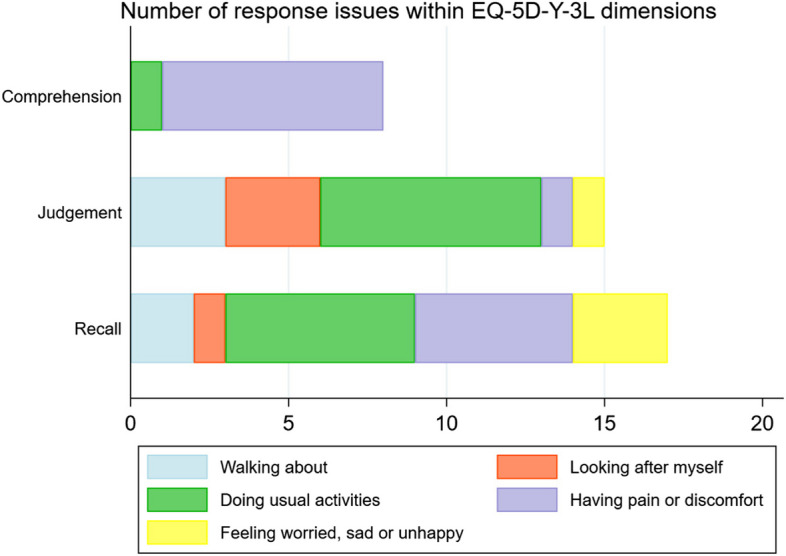
Overall, response issues were detected in n = 18 (46%) children. Comprehension issues were apparent in the "having pain or discomfort" dimension where children found it challenging to understand 'discomfort'. Recall-related issues were observed where children's responses were influenced by their typical tendencies (e.g., being usually worried) or past incidences (e.g., feeling pain sometimes). Judgement-related issues were the most common, particularly in the "doing usual activities" dimension, where children tended to respond based on their self-perceived ability to engage in activities rather than health-related limitations. None of the participants were found to have problems with response mapping. A healthy lifestyle that included diet and exercise was a notable consideration in EQ VAS ratings. The younger age groups had a higher proportion of response issues (6-7 years: 64%, 8-10 years: 62%), compared to older children (11-12 years: 20%). Moreover, children with response issues demonstrated significantly lower EQ-5D-Y-3L scores (mean = 0.78, se = 0.04) as compared to those without (mean = 0.95, se = 0.02) (p-value < 0.001). The overall inter-rater agreement was higher for those without any response issues (CCC = 0.33) than those with (CCC = 0.14). Additionally, higher agreement was noted across all the five dimensions in the subgroup with no response issues relative to those with.
Children in the general community may have different perceptions of HRQoL when responding to the EQ-5D-Y-3L possibly due to their limited experience with health-related challenges. The retrospective think-aloud approach adopted highlighted the relatively higher prevalence of response issues in the younger children (ages < 11 years), indicating the need for careful interpretation of self-reported HRQoL using the current version of the EQ-5D-Y-3L in this population.
EQ-5D-Y-3L被广泛用于测量和评估儿童群体的健康相关生活质量(HRQoL)。这项混合方法研究使用了EQ-5D-Y-3L测量工具,并采用回顾性出声思维法来检验不同实足年龄儿童的自我报告有效性。
在一个基于社区的39名6至12岁儿童样本中进行了一项混合方法研究。在半结构式访谈中,儿童自行完成EQ-5D-Y-3L,然后进行回顾性出声思维。对话被录音并转录,以便在NVivo中使用图兰乔四阶段反应模型框架进行分析,以评估理解、判断、回忆和反应映射问题。使用费舍尔精确检验来评估各亚组儿童自我报告的HRQoL之间的差异。儿童与父母二元组之间的评分者间一致性通过总体HRQoL的组内相关系数(CCC)和维度水平HRQoL的格韦特AC系数进行评估。
总体而言,在n = 18名(46%)儿童中检测到反应问题。理解问题在“有疼痛或不适”维度中很明显,儿童发现理解“不适”具有挑战性。观察到与回忆相关的问题,即儿童的回答受到其典型倾向(如通常担心)或过去事件(如有时感到疼痛)的影响。与判断相关的问题最为常见,特别是在“进行日常活动”维度中,儿童倾向于根据自己参与活动的自我感知能力而非与健康相关的限制来做出回答。未发现参与者在反应映射方面存在问题。包括饮食和锻炼在内的健康生活方式是EQ视觉模拟量表(VAS)评分中的一个显著考虑因素。与年龄较大的儿童(11至12岁:20%)相比,年龄较小的组反应问题的比例更高(6至7岁:64%,8至10岁:62%)。此外,与没有反应问题的儿童(平均值 = 0.95,标准误 = 0.02)相比,有反应问题的儿童EQ-5D-Y-3L得分显著更低(平均值 = 0.78,标准误 = 0.04)(p值 < 0.001)。对于没有任何反应问题的儿童,总体评分者间一致性(CCC = 0.33)高于有反应问题的儿童(CCC = 0.14)。此外,在没有反应问题的亚组中,所有五个维度的一致性相对于有反应问题的亚组更高。
普通社区中的儿童在回答EQ-5D-Y-3L时可能对HRQoL有不同的认知,这可能是由于他们在与健康相关挑战方面的经验有限。所采用的回顾性出声思维法突出了年幼儿童(年龄 < 11岁)中反应问题的相对较高发生率,表明在该人群中使用当前版本的EQ-5D-Y-3L对自我报告的HRQoL进行仔细解释的必要性。