Department of Psychiatry, Section Medical Psychology and Psychotherapy, Erasmus MC University Medical Center, Wytemaweg 80, 3015 CN, Rotterdam, The Netherlands.
Faculty of Psychology, YARSI University, Jakarta, Indonesia.
Health Qual Life Outcomes. 2022 Jun 3;20(1):88. doi: 10.1186/s12955-022-01996-w.
Self-report is the standard for measuring people's health-related quality of life (HRQoL), including children. However, in certain circumstances children cannot report their own health. For this reason, children's HRQoL measures often provide both a self-report and a proxy-report form. It is not clear whether the measurement properties will be the same for these two forms. We investigated whether it would be beneficial to extend the classification system of the EQ-5D-Y proxy questionnaire from 3 to 5 response levels. The agreement between self-report and proxy-report was assessed for both EQ-5D-Y measures.
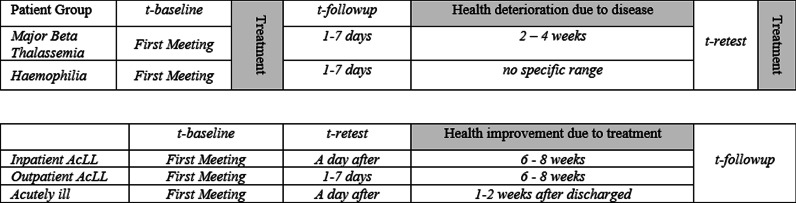
The study included 286 pediatric patients and their caregivers as proxies. At three consecutive measurements-baseline, test-retest and follow-up-the proxies assessed the child's HRQoL using the EQ-5D-Y-3L, EQ-5D-Y-5L, the PedsQL Generic, and matched disease-specific instruments. The proxy versions of EQ-5D-Y-3L and EQ-5D-Y-5L were compared in terms of feasibility, distribution properties, convergent validity, test-retest and responsiveness. Agreement between both EQ-5D-Y proxy versions to their respective self-report versions was assessed at baseline and follow-up.
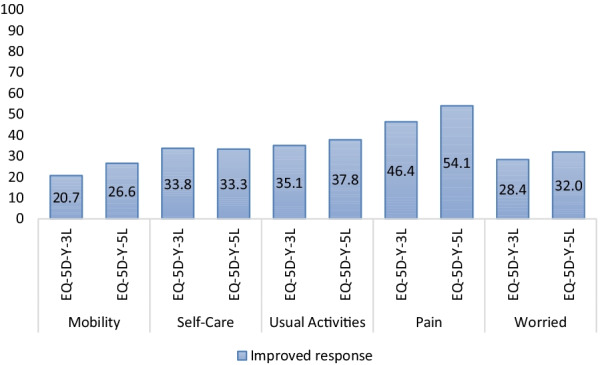
The proportion of missing responses was 1% for the EQ-5D-Y-3L and 1.4% for the EQ-5D-Y-5L. The frequency of health state with no problems in all dimensions (11111) was slightly lower for the EQ-5D-Y-5L (21.3% vs 16.7%). Regarding the convergent validity with the PedsQL and disease-specific measures, the proxy versions of EQ-5D-Y-3L and EQ-5D-Y-5L had similar magnitudes of associations between similar dimensions. The means of test-retest coefficients between the two versions of the EQ-5D-Y proxy were comparable (0.83 vs. 0.84). Regarding reported improved conditions, responsiveness of the EQ-5D-Y-5L proxy (26.6-54.1%) was higher than that of the EQ-5D-Y-3L proxy (20.7-46.4%). Except for acutely ill patients, agreement between the EQ-5D-Y-5L proxy and self-reports was at least moderate.
Extending the number of levels of the proxy version of EQ-5D-Y can improve the classification accuracy and the ability to detect health changes over time. The level structure of EQ-5D-Y-5L was associated with a closer agreement between proxy and self-report. The study findings support extending the EQ-5D-Y descriptive system from 3 to 5 levels when administered by a proxy, which is often the case in the pediatric population.
自我报告是衡量人们健康相关生活质量(HRQoL)的标准,包括儿童。然而,在某些情况下,儿童无法报告自己的健康状况。出于这个原因,儿童 HRQoL 测量通常提供自我报告和代理报告两种形式。目前还不清楚这两种形式的测量属性是否相同。我们研究了将 EQ-5D-Y 代理问卷的分类系统从 3 级扩展到 5 级是否会有帮助。评估了两种 EQ-5D-Y 测量方法的自我报告和代理报告之间的一致性。
本研究纳入了 286 名儿科患者及其作为代理的看护人。在连续三次测量(基线、测试-重测和随访)中,代理使用 EQ-5D-Y-3L、EQ-5D-Y-5L、PedsQL 通用和匹配的疾病特异性仪器评估儿童的 HRQoL。比较了 EQ-5D-Y-3L 和 EQ-5D-Y-5L 的代理版本在可行性、分布特性、收敛效度、测试-重测和反应性方面的差异。在基线和随访时,评估了两种 EQ-5D-Y 代理版本与各自的自我报告版本之间的一致性。
EQ-5D-Y-3L 的缺失率为 1%,EQ-5D-Y-5L 的缺失率为 1.4%。EQ-5D-Y-5L 中所有维度均无问题的健康状态频率(11111)略低(21.3% vs 16.7%)。关于与 PedsQL 和疾病特异性测量的收敛效度,EQ-5D-Y-3L 和 EQ-5D-Y-5L 代理版本之间相似维度的关联具有相似的大小。两个版本的 EQ-5D-Y 代理版本的测试-重测系数平均值相当(0.83 vs. 0.84)。关于报告的改善情况,EQ-5D-Y-5L 代理的反应性(26.6-54.1%)高于 EQ-5D-Y-3L 代理的反应性(20.7-46.4%)。除急性病患者外,EQ-5D-Y-5L 代理与自我报告之间的一致性至少为中度。
扩展 EQ-5D-Y 代理版本的等级数量可以提高分类准确性和随时间检测健康变化的能力。EQ-5D-Y-5L 的等级结构与代理和自我报告之间更紧密的一致性相关。研究结果支持在儿科人群中,当由代理进行 EQ-5D-Y 描述性系统从 3 级扩展到 5 级。