Singh Awadhesh Kumar, Das Ashok Kumar, Murthy L Sreenivasa, Ghosal Samit, Sahay Rakesh, Harikumar K V S, Keshava Ganesh Hosahithlu, Agarwal Mayur, Vijayakumar G, Kalra Pramila, Lodha Piyush, Das Sambit, Shaikh Shehla, Goswami Soumik, Ajish T P, Kumthekar Prashant, Upadhyay Mihir, Thamburaj Anthuvan, Mahule Aushili, Prasad Ashish, Pednekar Abhijit
GD Hospital and Diabetes Institute, 139 A, Lenin Sarani Rd, Bowbazar, Kolkata, West Bengal, 700013, India.
Mahatma Gandhi Medical College, Cuddalore Rd, ECR, Pillayarkuppam, Puducherry, 607402, India.
Adv Ther. 2025 Feb;42(2):801-812. doi: 10.1007/s12325-024-03037-y. Epub 2024 Dec 5.
A slower adoption rate of fixed dose combinations (FDC) in diabetes management is partly due to insufficient data. This study evaluates the safety and efficacy of an FDC of dapagliflozin + sitagliptin + metformin hydrochloride extended release (XR), compared to a dual FDC of sitagliptin + metformin hydrochloride XR among patients with type 2 diabetes mellitus (T2DM) with poor glycemic control when treated with metformin monotherapy.
A total of 274 patients with T2DM were randomized (1:1) to either arm X, receiving FDC of dapagliflozin (10 mg) + sitagliptin (100 mg) + metformin hydrochloride XR (1000 mg) (Dapa + Sita + Met) tablets, or arm Y, receiving sitagliptin phosphate (100 mg) + metformin hydrochloride XR (1000 mg) (Sita + Met) tablets, and treated for 16 weeks. The outcome measures included changes in hemoglobin A1c (HbA1c)(%), fasting plasma glucose (FPG), 2-h post-prandial glucose (PPG), weight, and the proportion of patients achieving target HbA1c levels of < 7.0% by week 16 of the study period.
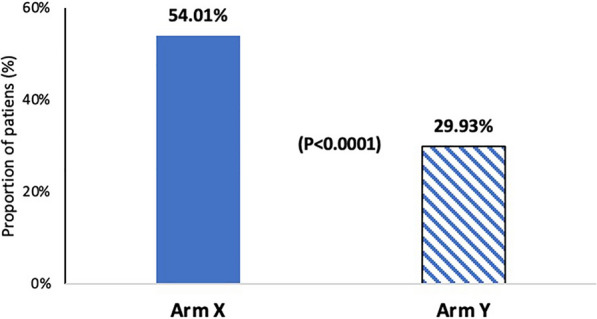
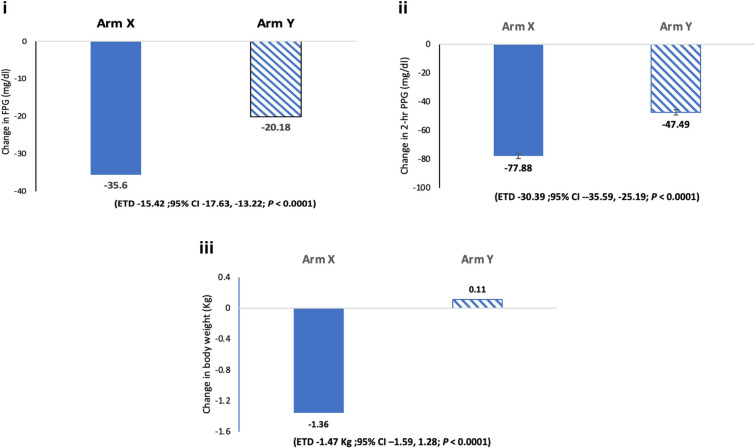
The reduction in HbA1c at week 16 was significantly higher in arm X than in arm Y [estimated treatment difference (ETD), - 0.65% (95% CI - 0.76 to - 0.53; P < 0.0001)]. Arm X showed a marked decrease in FPG [ETD - 15.42 mg/dl; 95% CI (17.63, 13.22; P < 0.0001)], PPG [ETD - 30.39 mg/dl; 95% CI (35.59, 25.19; P < 0.0001)], and weight [ETD - 1.47 kg; 95% CI (1.59, 1.28; P < 0.0001)] after 16 weeks. In arm X, 54% of patients reached HbA1c < 7.0% compared to 29.9% in arm Y. The incidence of adverse events was comparable [13.14% (arm X) vs 12.4% (arm Y)]. There was no severe hypoglycemia-led treatment discontinuation.
Among patients with T2DM who have poor glycemic control with metformin monotherapy, triple FDC (Dapa + Sita + Met) effectively helped achieve better glycemic response compared to dual FDC (Sita + Met), with a comparable safety and tolerability profile.
CTRI/2022/01/039857.
固定剂量复方制剂(FDC)在糖尿病管理中的采用率较低,部分原因是数据不足。本研究评估了达格列净+西他列汀+盐酸二甲双胍缓释片(XR)的FDC与西他列汀+盐酸二甲双胍缓释片的双联FDC相比,在接受二甲双胍单药治疗血糖控制不佳的2型糖尿病(T2DM)患者中的安全性和有效性。
总共274例T2DM患者被随机(1:1)分为X组,接受达格列净(10mg)+西他列汀(100mg)+盐酸二甲双胍缓释片(1000mg)(Dapa+Sita+Met)片剂,或Y组,接受磷酸西他列汀(100mg)+盐酸二甲双胍缓释片(1000mg)(Sita+Met)片剂,并治疗16周。结局指标包括糖化血红蛋白(HbA1c)(%)、空腹血糖(FPG)、餐后2小时血糖(PPG)、体重的变化,以及在研究期第16周时达到HbA1c水平<7.0%的患者比例。
第16周时,X组HbA1c的降低显著高于Y组[估计治疗差异(ETD),-0.65%(95%CI-0.76至-0.53;P<0.0001)]。X组在16周后FPG[ETD-15.42mg/dl;95%CI(17.63,13.22;P<0.0001)]、PPG[ETD-30.39mg/dl;95%CI(35.59,25.19;P<0.0001)]和体重[ETD-1.47kg;95%CI(1.59,1.