Lara-Reyna Jacques, Karabacak Mert, Wedderburn Raymond, Legome Eric, Margetis Konstantinos
Department of Neurosurgery, University of Illinois College of Medicine, Peoria, United States.
Department of Neurosurgery, Mount Sinai Health System, New York, United States.
Surg Neurol Int. 2024 Nov 29;15:437. doi: 10.25259/SNI_389_2024. eCollection 2024.
This study primarily aimed to assess the volumetric attributes of the midbrain and perimesencephalic structures preoperatively and following surgical interventions in patients diagnosed with brain herniation secondary to traumatic brain injury (TBI).
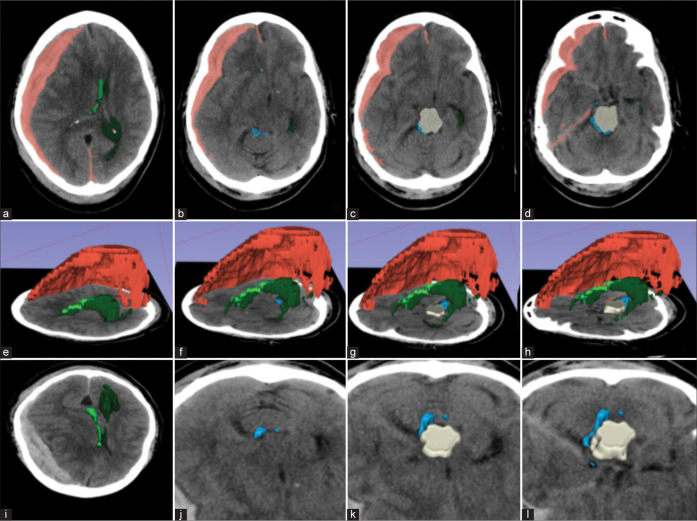
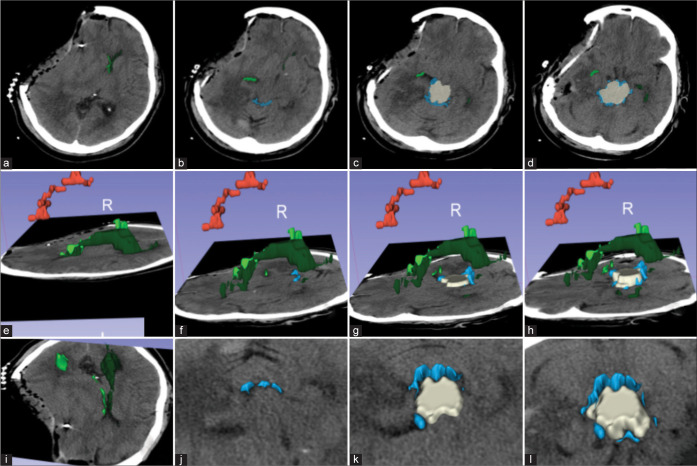
We evaluated patients based on radiological findings and clinical symptoms indicative of brain herniation. We performed semi-automated segmentation of the intracranial structures most relevant to trauma and of interest for the current study, such as hematoma, ventricles, midbrain, and perimesencephalic cisterns. Using preoperative and postoperative computed tomography scans, we measured and analyzed the volume of these structures. Patients were grouped based on their discharge Glasgow Coma Scale (GCS) scores: GCS 15 and non-GCS 15.
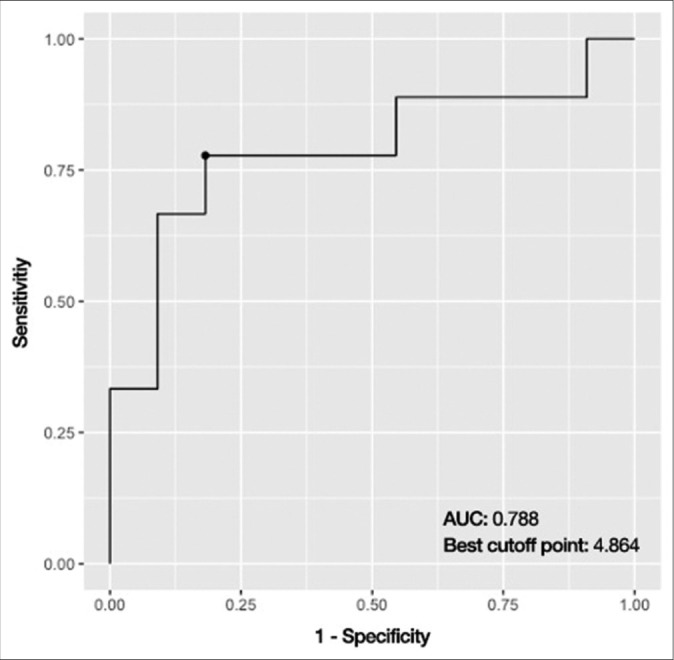
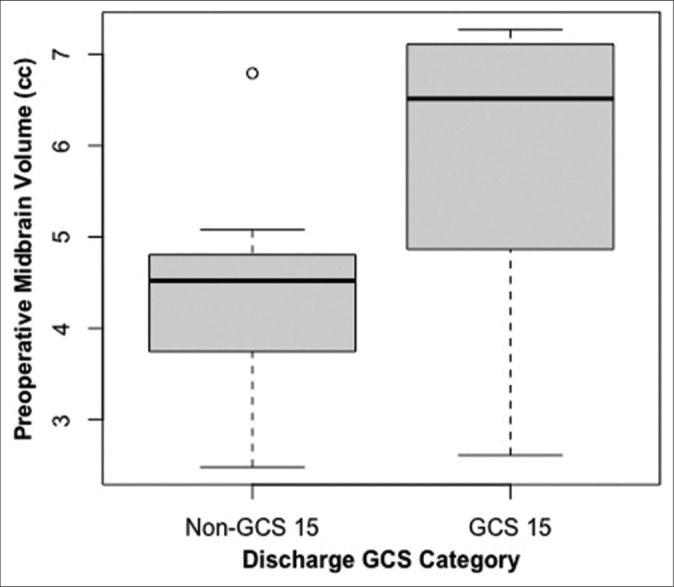
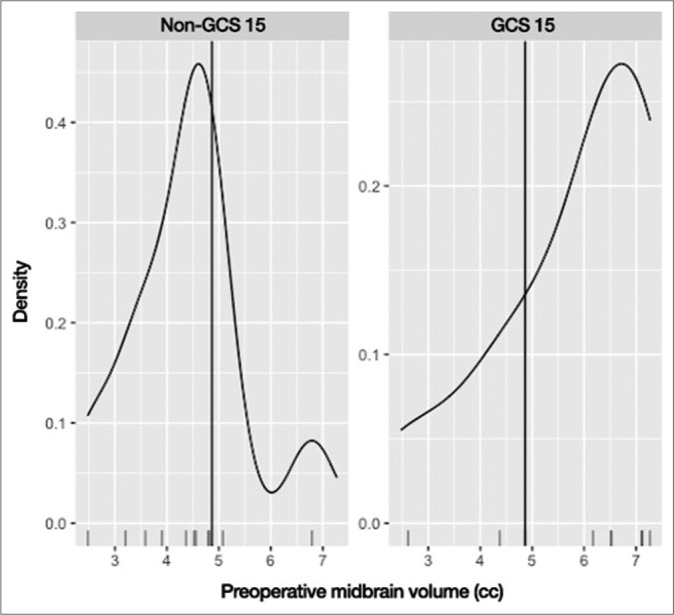
From May 2018 to February 2020, we included 20 patients in the study. Our volumetric analysis revealed that preoperative midbrain volume (5.84 cc vs. 4.37 cc, = 0.034) was a significant differentiator between GCS 15 and non-GCS 15 groups. Preoperative midbrain volume remained significant in univariate (odds ratio [OR] = 2.280, 95% confidence interval (CI) = 1.126-5.929, = 0.04) and multivariate logistic regression analysis (adjusted OR = 3.204, 95% CI = 1.228-12.438, = 0.038) even after adjusting for age, sex, and admission GCS score. We identified a cut-off point of 4.86 ccs in preoperative midbrain volume, which demonstrated a discriminatory performance of 0.788 area under the receiver operating characteristic curve, 80.0% accuracy, 77.8% sensitivity, and 81.8% specificity between the two groups.
Our findings suggest that patients presenting with lesser midbrain compression preoperatively tended to have improved clinical outcomes postsurgery. Thus, we propose that this preoperative midbrain volume cut-off point holds predictive value for clinical outcomes within our cohort.
本研究的主要目的是评估创伤性脑损伤(TBI)继发脑疝患者术前及手术干预后脑干和中脑周围结构的容积属性。
我们根据提示脑疝的影像学表现和临床症状对患者进行评估。我们对与创伤最相关且本研究感兴趣的颅内结构进行半自动分割,如血肿、脑室、中脑和中脑周围脑池。利用术前和术后计算机断层扫描,我们测量并分析了这些结构的容积。患者根据出院时的格拉斯哥昏迷量表(GCS)评分分组:GCS 15分和非GCS 15分。
从2018年5月至2020年2月,我们纳入了20例患者进行研究。我们的容积分析显示,术前中脑容积(5.84立方厘米对4.37立方厘米,P = 0.034)是GCS 15分和非GCS 15分组之间的显著差异因素。即使在调整年龄、性别和入院时GCS评分后,术前中脑容积在单因素(优势比[OR]=2.280,95%置信区间[CI]=1.126 - 5.929,P = 0.04)和多因素逻辑回归分析中(调整后OR = 3.204,95%CI = 1.228 - 12.438,P = 0.038)仍具有显著性。我们确定术前中脑容积的截断点为4.86立方厘米,其在两组之间的受试者操作特征曲线下面积为0.788,准确率为80.0%,敏感性为77.8%,特异性为81.8%。
我们的研究结果表明,术前中脑受压较轻的患者术后临床结局往往较好。因此,我们提出这个术前中脑容积截断点对我们队列中的临床结局具有预测价值。