Zhuang Si-Dian, Bao Zhe-Yan, Tang Xiao-Mei, Xiang Jiao, Mo Chan, Zhong Shui-Sheng
Department of Neurology, Guangdong Sanjiu Brain Hospital, Guangzhou, Guangdong, China.
BMC Neurol. 2024 Dec 6;24(1):476. doi: 10.1186/s12883-024-03984-7.
Anti-IgLON5 disease is a rare autoimmune mediated disease. It is mainly featured by sleep-related disturbance, parkinsonism, chorea and limb ataxia. Previous studies had clarified its clinical manifestations and predisposing genes. However, as far as we know, anti-IgLON5 disease combined with paraneoplastic cerebellar degeneration (PCD) with the detection of anti-Sulfatide IgG antibody, masquerading as meningoencephalitis had not been reported before.
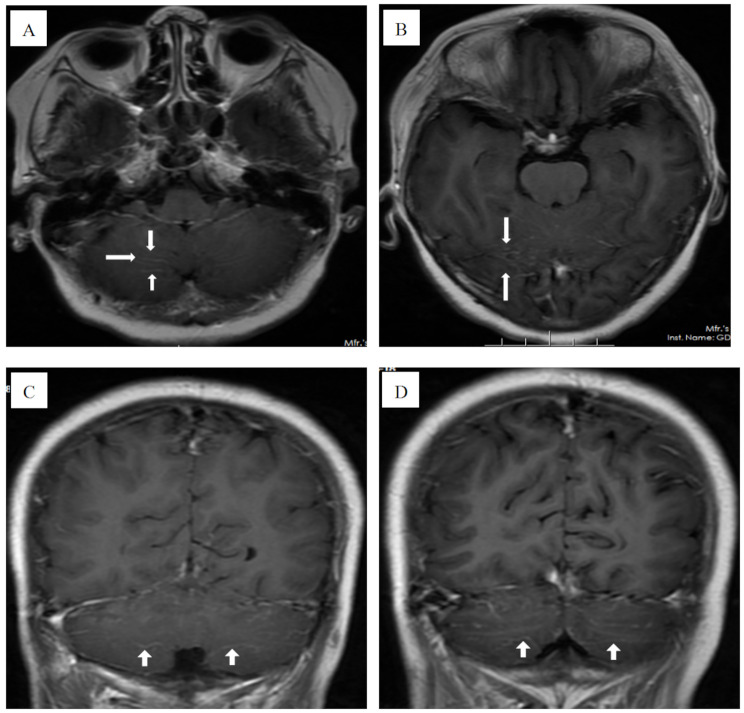
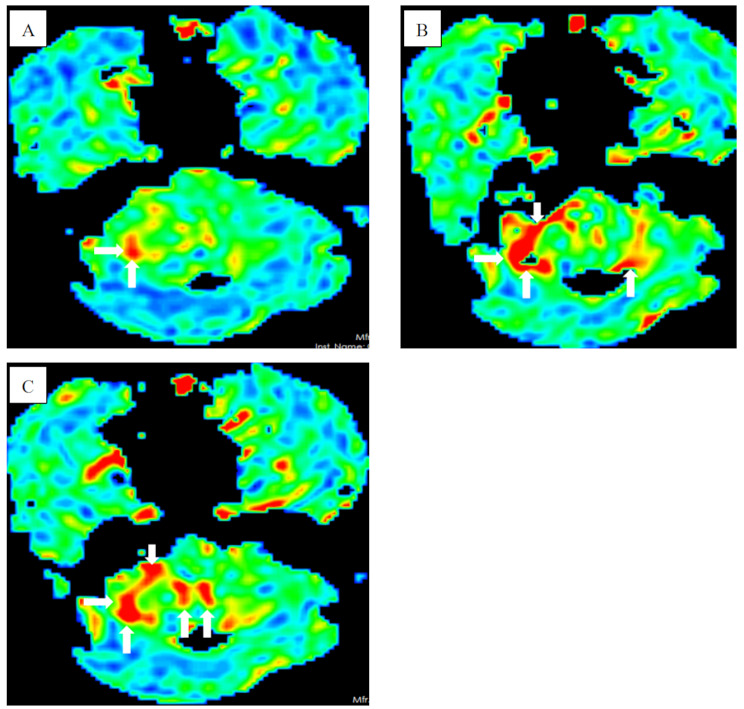
A 57-year-old Chinese female presented with walking unsteadily for 12 days and logagnosia for 2 days and was admitted to our hospital. She had a past history of breast cancer. Magnetic resonance imaging (MRI) revealed leptomeningeal enhancement (prominent in cerebellar hemisphere). Arterial spin labeling (ASL) perfusion showed hyperperfusion in the cerebellar hemisphere and interhemispheric fissure cistern. MRI and ASL indicated the diagnosis was meningoencephalitis. However, IgG anti-IgLON5 antibody was positive in both serum and cerebrospinal fluid. Therefore, the diagnosis was anti-IgLON5 disease. In addition, the patient combined with PCD due to positive anti-Yo-antibody in serum fluid .
Whereas sleep disturbance is the most common feature in patients with anti-IgLON5 disease, our case presented with walking unsteadily and logagnosia. Anti-IgLON5 disease combined with PCD with the detection of anti-Sulfatide IgG antibody, masquerading as meningoencephalitis is very rare. Therefore, if meningoencephalitis did not recover with conventional treatment, anti-IgLON5 disease and PCD should be considered as the differential diagnosis.
抗IgLON5病是一种罕见的自身免疫介导性疾病。其主要特征为睡眠相关障碍、帕金森综合征、舞蹈症和肢体共济失调。既往研究已阐明其临床表现和易感基因。然而,据我们所知,抗IgLON5病合并副肿瘤性小脑变性(PCD)并检测到抗硫脂IgG抗体,伪装成脑膜脑炎此前尚未见报道。
一名57岁中国女性因行走不稳12天、言语失认2天入院。她有乳腺癌病史。磁共振成像(MRI)显示软脑膜强化(小脑半球明显)。动脉自旋标记(ASL)灌注显示小脑半球和大脑镰裂池血流灌注增加。MRI和ASL提示诊断为脑膜脑炎。然而,血清和脑脊液中IgG抗IgLON5抗体均为阳性。因此,诊断为抗IgLON5病。此外,患者因血清中抗Yo抗体阳性合并PCD。
虽然睡眠障碍是抗IgLON5病患者最常见的特征,但我们的病例表现为行走不稳和言语失认。抗IgLON5病合并PCD并检测到抗硫脂IgG抗体,伪装成脑膜脑炎非常罕见。因此,如果脑膜脑炎经传统治疗未恢复,应考虑抗IgLON5病和PCD进行鉴别诊断。