Philipps Jörg, Knaup Mark, Katz Maria, Axton Konrad, Mork Hannah, Treichel Jasmin, Lüling Benjamin, Klimas Rafael, Wille Kai, Schellinger Peter Dieter, Pitarokoili Kalliopi
Department of Neurology and Neurogeriatrics, Johannes Wesling Klinikum Minden, Ruhr-University Bochum, Minden, Germany.
Department of Neurology, St. Josef-Hospital, Ruhr-University Bochum, Bochum, Germany.
J Neuroimaging. 2025 Jan-Feb;35(1):e13255. doi: 10.1111/jon.13255.
The role of high-resolution nerve ultrasound (HRUS) in the diagnosis of chemotherapy-induced polyneuropathy is unclear. The present prospective longitudinal controlled study evaluates the utility of HRUS in vincristine-induced polyneuropathy (VIPN).
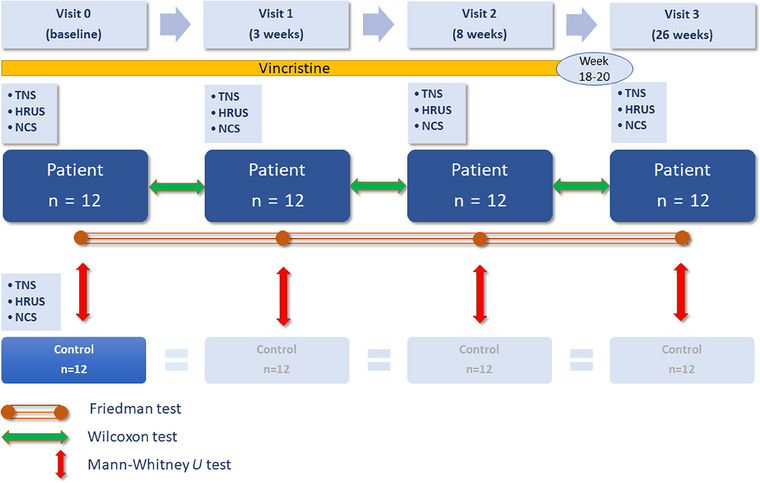
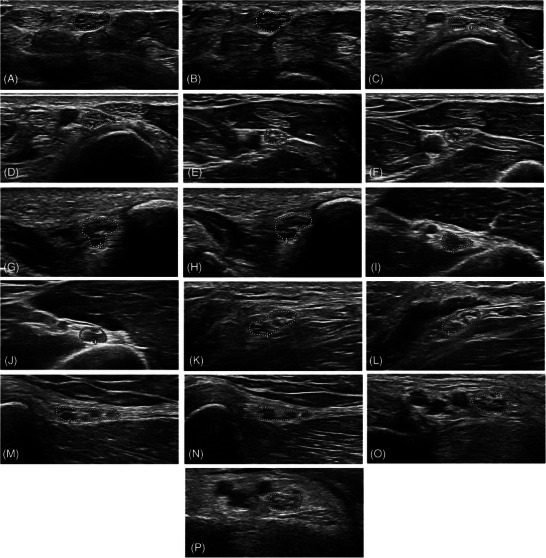
Twelve patients receiving vincristine and 12 healthy age-matched controls were included. Visits before and 3 weeks, 8 weeks, and 6 months after the start of vincristine treatment included clinical examination, the total neuropathy score (TNS), nerve conduction studies (NCSs), and HRUS of the bilateral median, ulnar, radial, tibial, peroneal, and sural nerve cross-sectional areas (CSAs).
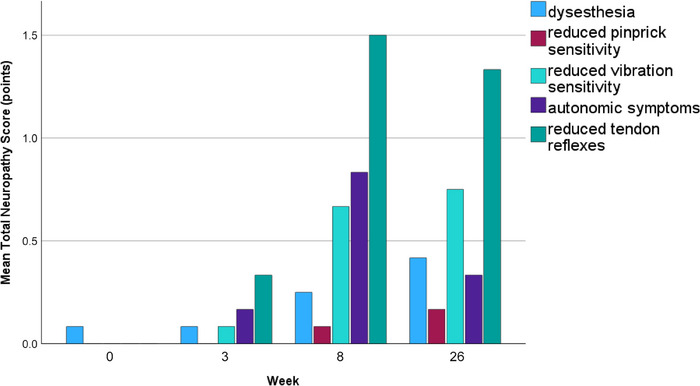
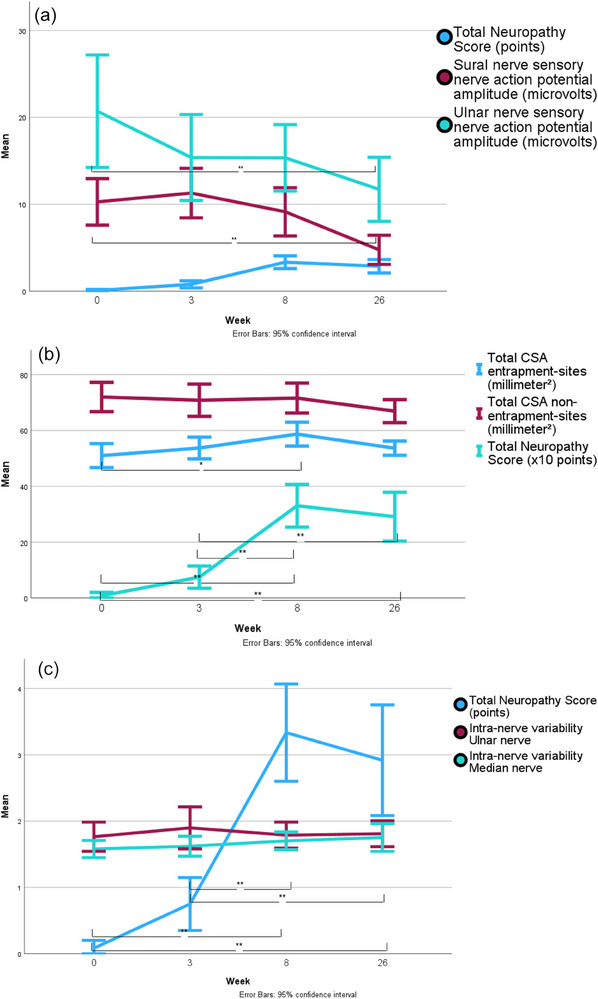
Median TNS increased from 0 points (interquartile range [IQR] 0) to 0.5 points (IQR 1, p = .26) at Week 3 and to 4 points (IQR 2.5, p < .001) at Week 8. At 6 months, there was a nonsignificant decrease to 2 points (IQR 2, p = .66). HRUS of individual nerve sites showed no significant changes in CSA and intranerve variability. The total CSA of all entrapment sites increased significantly (p = .007) at Week 8. Sensory nerve action potentials decreased significantly after 6 months (sural nerve, p = .001; radial nerve, p = .004; ulnar and median nerve, p < .001). The tibial nerve compound muscle action potential (p = .006) and nerve conduction velocity (p < .001) were reduced.
At mid-treatment, there is an increase in the total CSA at entrapment sites parallel to an increase in clinical symptoms. In individual nerve sites, HRUS does not detect significant signs of VIPN. NCSs exhibit signs of a predominantly sensory axonal polyneuropathy. The clinical examination remains the most sensitive tool in the early detection of VIPN.
高分辨率神经超声(HRUS)在化疗诱导的多发性神经病诊断中的作用尚不清楚。本前瞻性纵向对照研究评估了HRUS在长春新碱诱导的多发性神经病(VIPN)中的应用价值。
纳入12例接受长春新碱治疗的患者和12例年龄匹配的健康对照。在长春新碱治疗开始前、治疗3周、8周和6个月时进行访视,包括临床检查、总神经病变评分(TNS)、神经传导研究(NCS)以及对双侧正中神经、尺神经、桡神经、胫神经、腓总神经和腓肠神经横截面积(CSA)的HRUS检查。
第3周时,TNS中位数从0分(四分位间距[IQR]为0)增至0.5分(IQR为1,p = 0.26),第8周时增至4分(IQR为2.5,p < 0.001)。6个月时,降至2分(IQR为2,p = 0.66),差异无统计学意义。各神经部位的HRUS检查显示CSA和神经内变异性无显著变化。第8周时所有卡压部位的总CSA显著增加(p = 0.007)。6个月后感觉神经动作电位显著降低(腓肠神经,p = 0.001;桡神经,p = 0.004;尺神经和正中神经,p < 0.001)。胫神经复合肌肉动作电位(p = 0.006)和神经传导速度(p < 0.001)降低。
治疗中期,卡压部位的总CSA增加,同时临床症状加重。在单个神经部位,HRUS未检测到VIPN的明显体征。NCS显示主要为感觉轴索性多发性神经病的体征。临床检查仍是早期检测VIPN最敏感的工具。