Leng Songyao, Cao Li, Wang Xingru, Chen Jian, Wang Xiaojun, Cao Yong, Li Xuesong, Zheng Shuguo, Tian Feng, Li Jianwei
Department of Hepatobiliary Surgery, Southwest Hospital, Army Medical University, Chongqing, People's Republic of China.
Department of General Surgery, The First People's Hospital of Neijiang, Neijiang, Sichuan, People's Republic of China.
J Hepatocell Carcinoma. 2024 Dec 5;11:2413-2425. doi: 10.2147/JHC.S483014. eCollection 2024.
The objective of this study was to investigate the long-term outcomes between laparoscopic anatomical liver resection (LAR) and laparoscopic non-anatomical liver resection (LNAR) in patients with hepatocellular carcinoma (HCC).
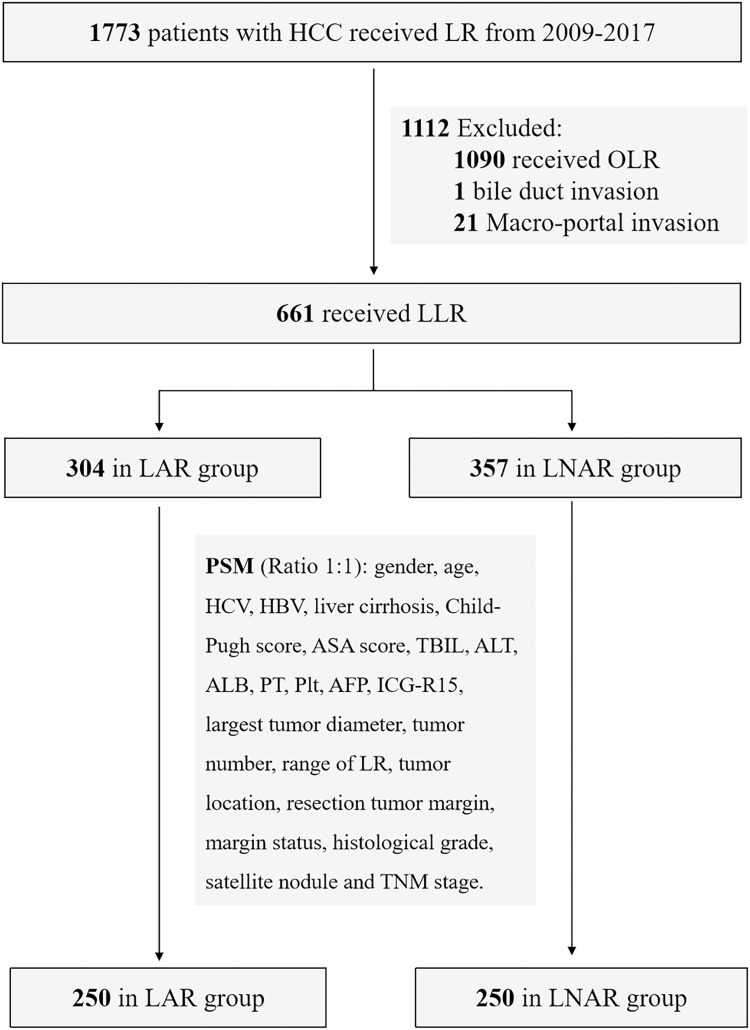
In this single-center retrospective cohort study, 1773 patients, from January 2009 to December 2017, were assessed for inclusion. After exclusions, 661 patients were included: 304 patients received LAR and 357 patients received LNAR. Propensity score matching (PSM) with 1:1 ratio was used to eliminate the selection bias between LAR and LNAR groups. The Kaplan-Meier and Cox models were used for survival analysis.
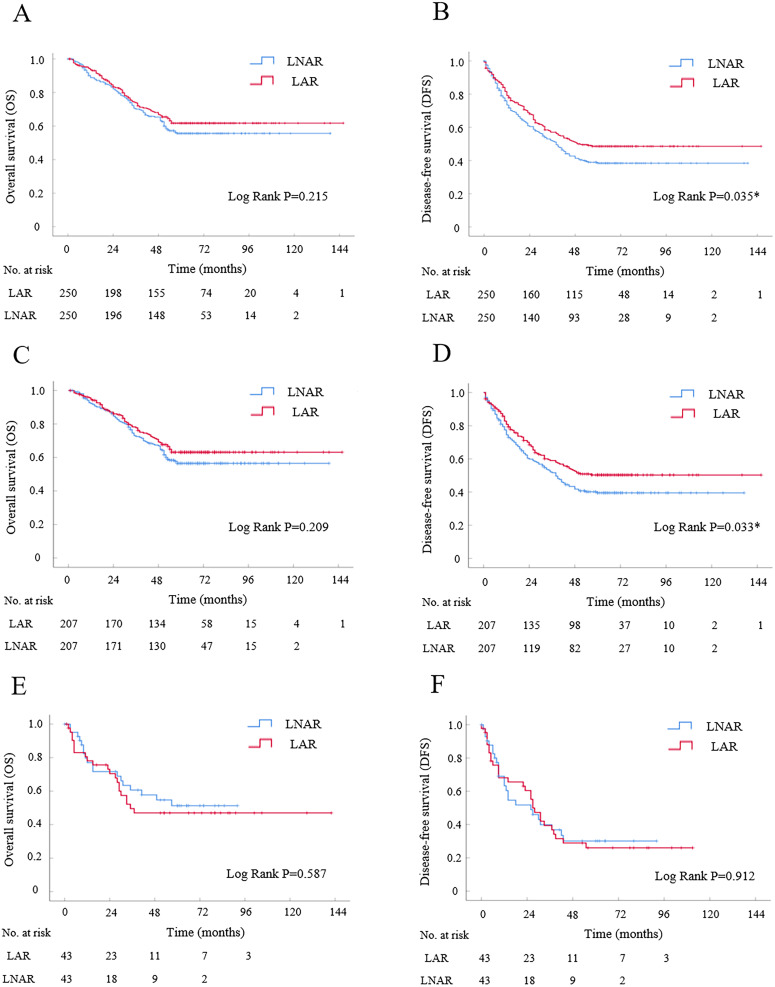
After PSM, 250 patients were in LAR or LNAR group, respectively. The overall survival (OS) had no significant difference between LAR and LNAR by Kaplan-Meier analysis. While, LAR had better disease-free survival (DFS) compared with LNAR (Log-rank P=0.035). The cumulative 5-year DFS rates were 48% for LAR, and 38% for LNAR. By Cox analysis, LAR was an independent risk factor of DFS (HR=1.308, P=0.030). In subgroup analysis for tumor size ≤ 5 cm, 207 patients were in LAR or LNAR subgroup after PSM. LAR had better DFS compared with LNAR (Log-rank P=0.033). LAR was an independent risk factor of DFS (HR=1.333, P=0.036). The cumulative 5-year DFS rates were 50% for LAR, and 39% for LNAR. In another subgroup analysis for tumor size > 5 cm, 43 patients were in LAR or LNAR subgroup after PSM. The DFS had no significant difference between LAR and LNAR (Log-rank P=0.912).
LAR is preferred for HCC patients with tumor size ≤5cm compared with LNAR because of the better DFS. For patients with tumor size >5cm, LAR and LNAR might be alternative procedures with comparable long-term outcomes.
本研究旨在探讨肝细胞癌(HCC)患者接受腹腔镜解剖性肝切除(LAR)与腹腔镜非解剖性肝切除(LNAR)后的长期预后情况。
在这项单中心回顾性队列研究中,对2009年1月至2017年12月期间的1773例患者进行纳入评估。排除相关病例后,共纳入661例患者:304例接受LAR,357例接受LNAR。采用1:1比例的倾向评分匹配(PSM)来消除LAR组和LNAR组之间的选择偏倚。采用Kaplan-Meier法和Cox模型进行生存分析。
PSM后,LAR组和LNAR组各有250例患者。Kaplan-Meier分析显示,LAR组和LNAR组的总生存期(OS)无显著差异。然而,LAR组的无病生存期(DFS)优于LNAR组(Log秩检验P = 0.035)。LAR组和LNAR组的5年累积DFS率分别为48%和38%。Cox分析显示,LAR是DFS的独立危险因素(HR = 1.308,P = 0.030)。在肿瘤大小≤5 cm的亚组分析中,PSM后LAR亚组和LNAR亚组各有207例患者。LAR组的DFS优于LNAR组(Log秩检验P = 0.033)。LAR是DFS的独立危险因素(HR = 1.333,P = 0.036)。LAR组和LNAR组的5年累积DFS率分别为50%和39%。在另一项肿瘤大小>5 cm的亚组分析中,PSM后LAR亚组和LNAR亚组各有43例患者。LAR组和LNAR组的DFS无显著差异(Log秩检验P = 0.912)。
对于肿瘤大小≤5 cm的HCC患者,与LNAR相比,LAR因其更好的DFS而更受青睐。对于肿瘤大小>5 cm的患者,LAR和LNAR可能是具有相似长期预后的替代手术方式。