Jianxi Wang, Xiongfeng Zou, Zehao Zheng, Zhen Zhao, Tianyi Peng, Ye Lin, Haosheng Jin, Zhixiang Jian, Huiling Wang
The Second School of Clinical Medicine, Southern Medical University, Guangzhou, China.
Department of General Surgery, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
Front Oncol. 2022 Jul 19;12:930065. doi: 10.3389/fonc.2022.930065. eCollection 2022.
Indocyanine green fluorescence-guided laparoscopic hepatectomy (ICG-guided LH) is increasingly used for the treatment of hepatocellular carcinoma (HCC). However, whether ICG-guided LH can improve surgical outcomes remains unclear. This study aimed to investigate the short-term outcomes and survival outcomes of ICG-guided LH versus common laparoscopic hepatectomy (CLH) for HCC.
We conducted a retrospective analysis of 104 ICG-guided LH and 158 CLH patients from 2014 to 2020 at our center. To avoid selection bias, 81 ICG-guided LH and 81 CLH cases were analyzed after 1:1 propensity score matching (PSM). The baseline data and results were compared between the two groups.
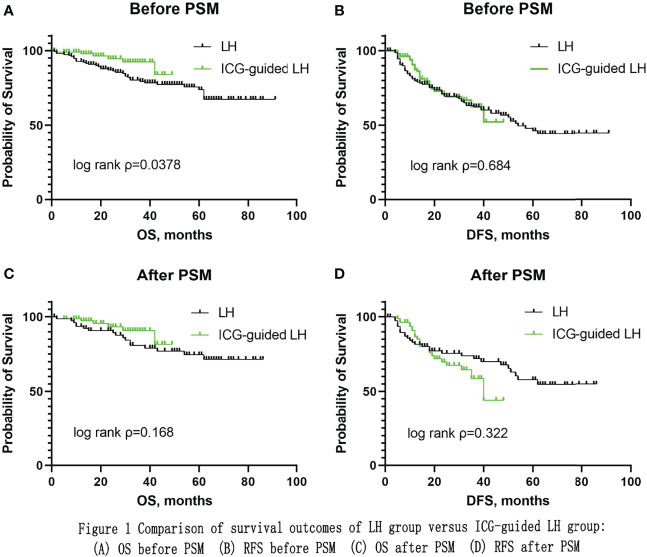
The baseline characteristics of both groups were comparable after matching. There was a significant difference in operative time: longer in the ICG-guided LH group than in the CLH group (p=0.004). However, there was no significant difference in operative time in anatomical resection between the two groups (p=0.987). There was a significant difference in operative time in non-anatomical resection: longer in the ICG-guided LH group than in the CLH group (p=0.001). There were no significant differences in positive surgery margin, blood loss, blood transfusion rate, postoperative complication rate, postoperative length of hospital stay, mortality within 30 days, and mortality within 90 days. The ICG-guided LH group appeared to have a trend towards better overall survival (OS), but there was no significant difference in OS (P=0.168) and recurrence-free survival (RFS) (P=0.322) between the two groups.
Although ICG fluorescence-guided LH is a timelier procedure to perform, it is a safe and effective technique with the advantages of intraoperative positioning, low postoperative complication rates, and potential to improve OS.
吲哚菁绿荧光引导下的腹腔镜肝切除术(ICG引导下的LH)越来越多地用于治疗肝细胞癌(HCC)。然而,ICG引导下的LH是否能改善手术效果仍不清楚。本研究旨在探讨ICG引导下的LH与普通腹腔镜肝切除术(CLH)治疗HCC的短期结局和生存结局。
我们对2014年至2020年在本中心接受治疗的104例ICG引导下的LH患者和158例CLH患者进行了回顾性分析。为避免选择偏倚,在1:1倾向评分匹配(PSM)后,对81例ICG引导下的LH病例和81例CLH病例进行了分析。比较两组的基线数据和结果。
匹配后两组的基线特征具有可比性。手术时间存在显著差异:ICG引导下的LH组比CLH组长(p=0.004)。然而,两组在解剖性切除中的手术时间无显著差异(p=0.987)。非解剖性切除的手术时间存在显著差异:ICG引导下的LH组比CLH组长(p=0.001)。手术切缘阳性、失血量、输血率、术后并发症发生率、术后住院时间、30天内死亡率和90天内死亡率方面无显著差异。ICG引导下的LH组似乎有总体生存(OS)更好的趋势,但两组在OS(P=0.168)和无复发生存(RFS)(P=0.322)方面无显著差异。
尽管ICG荧光引导下的LH是一种更及时的手术方法,但它是一种安全有效的技术,具有术中定位准确、术后并发症发生率低以及可能改善OS的优点。