Liu Chen Kiow Jeremy, Hoang Thomas, Bedi Harjot K, Majdzadeh Ardekani Zhina, Rosenfeld Daniel, Reise-Filteau Marica, Bressler Brian, Leung Yvette, Rosenfeld Greg
Department of Medicine, Division of Gastroenterology, Montreal University Hospital Centre (CHUM), Montreal H2X 3E4, Quebec, Canada.
Department of Gastroenterology, St. Paul's Hospital, Vancouver V6Z 1Y6, British Columbia, Canada.
World J Gastroenterol. 2024 Dec 14;30(46):4904-4913. doi: 10.3748/wjg.v30.i46.4904.
Over the last decade, the treatment options for inflammatory bowel disease (IBD) have significantly progressed with the emergence of new medications designed to target various immune pathways and mitigate inflammation. Adalimumab (ADA) is a tumor necrosis factor alpha antagonist and stands as an effective treatment for IBD. In April 2021, the province of British Columbia implemented a mandatory non-medical switch policy of the ADA originator Humira to ADA biosimilars. Biosimilars offer a potential cost-effective, safe, and efficacious alternative to the originator, yet there remains limited real-world evidence on long-term outcomes of ADA non-medical switching in IBD.
To assess the long-term outcomes of non-medical switching from the ADA originator Humira to an ADA biosimilar among IBD patients.
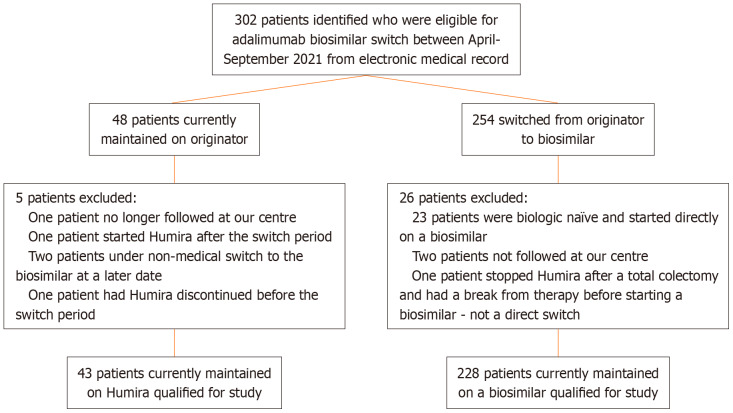
A retrospective observational chart review study was conducted on IBD patients eligible for the provincially mandated non-medical switch to an ADA biosimilar. The primary outcome was treatment persistence at 30 months post-switch. Secondary outcomes included the proportion of and reasons for therapy alteration or ADA discontinuation, loss of response (LOR) rates, adverse events (AE), and clinical and biochemical remission status. Patients who remained on the originator throughout the switch period, through compassionate support or private pay, constituted the comparison group.
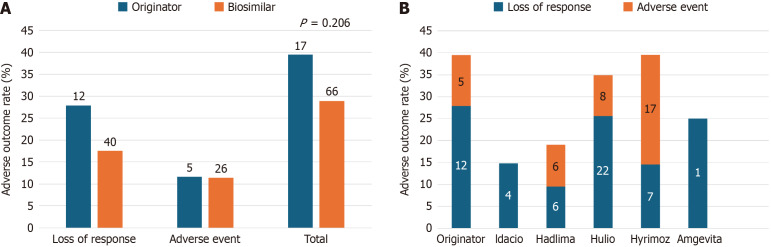
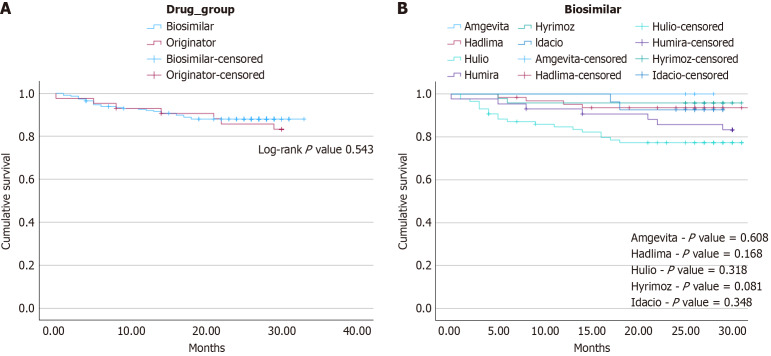
Patients in the originator ( = 43) and biosimilar switch ( = 228) groups displayed similar demographics and baseline disease characteristics. By the study endpoint of 30 months, there was no difference in the rate of treatment persistence in either group ( = 36, 83.7% originator group = 201, 88.2% biosimilar group, = 0.451). Treatment persistence demonstrated similar rates of discontinuation between both study groups (log-rank = 0.543). There was a numerical but not statistically significant difference in rates of adverse outcomes between either group (39.5% originator 28.9% biosimilars, = 0.206). This included comparable rates of LOR (27.9% 17.5%) or AE (11.6% 11.4%) between the originator and biosimilar cohorts, respectively. C-reactive protein and fecal calprotectin levels were similar one year pre- and post-switch.
These data support the long-term efficacy and safety of non-medical ADA switching in IBD and will help inform patients and physicians in jurisdictions currently undergoing biosimilar switching.
在过去十年中,随着旨在靶向各种免疫途径并减轻炎症的新药物的出现,炎症性肠病(IBD)的治疗选择有了显著进展。阿达木单抗(ADA)是一种肿瘤坏死因子α拮抗剂,是IBD的有效治疗药物。2021年4月,不列颠哥伦比亚省实施了一项强制性政策,将ADA原研药修美乐转换为ADA生物类似药。生物类似药为原研药提供了一种潜在的具有成本效益、安全且有效的替代方案,但关于IBD中ADA非医学转换的长期结果的真实世界证据仍然有限。
评估IBD患者从ADA原研药修美乐非医学转换为ADA生物类似药的长期结果。
对符合该省强制性非医学转换为ADA生物类似药条件的IBD患者进行了一项回顾性观察图表审查研究。主要结局是转换后30个月的治疗持续性。次要结局包括治疗改变或停用ADA的比例及原因、反应丧失(LOR)率、不良事件(AE)以及临床和生化缓解状态。在整个转换期间通过慈善支持或自费继续使用原研药的患者构成对照组。
原研药组(n = 43)和生物类似药转换组(n = 228)的患者在人口统计学和基线疾病特征方面相似。到30个月的研究终点时,两组的治疗持续率没有差异(原研药组n = 36,83.7%;生物类似药组n = 201,88.2%,P = 0.451)。治疗持续性显示两组之间的停药率相似(对数秩检验P = 0.543)。两组之间不良结局的发生率存在数值差异但无统计学意义(原研药组39.5%对生物类似药组28.9%,P = 0.206)。这包括原研药和生物类似药队列之间相似的LOR率(27.9%对17.5%)或AE率(11.6%对11.4%)。转换前后一年的C反应蛋白和粪便钙卫蛋白水平相似。
这些数据支持IBD中ADA非医学转换的长期疗效和安全性,并将有助于为目前正在进行生物类似药转换的地区的患者和医生提供信息。