Faidas Maria, Stockton Melissa A, Mphonda Steven M, Sansbury Griffin, Hedrick Haley, Devadas Jackson, Phanga Twambilile, Ruegsegger Laura, Kramer Jack, Mortensen Hillary, Kulisewa Kazione, Pence Brian W, Bhushan Nivedita L, Gaynes Bradley N
University of North Carolina at Chapel Hill, 321 S Columbia St., Chapel Hill, NC, 27599, USA.
University of Pennsylvania, Philadelphia, PA, USA.
BMC Glob Public Health. 2024 Jul 1;2(1):39. doi: 10.1186/s44263-024-00072-3.
In Malawi, approximately 25% of adolescents living with HIV (ALWH) also suffer from depression. Not only is HIV stigma a major contributor to depression but it also adversely impacts HIV care engagement. ALWH can experience HIV stigma as stereotyping, social exclusion, low social support, and abuse, and these experiences are associated with poor mental health. Despite recognition of the deleterious effects of HIV stigma, we have limited knowledge of how stigma is experienced by ALWH with comorbid depression. Guided by the Health Stigma and Discrimination Framework, we describe stigma faced by ALWH and comorbid depression in Malawi and its implications for future interventions.
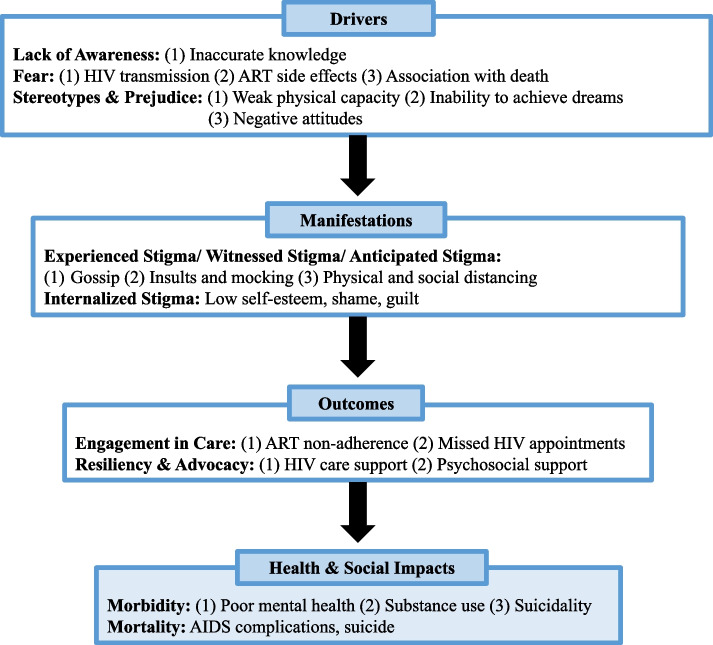
As part of a larger formative study to adapt a mental health counseling intervention, we conducted in-depth interviews, social support mapping sessions, and focus-group discussions with 25 ALWH, 4 caregivers of ALWH, 3 HIV providers, and 5 participants and 5 staff of a prior mental health counseling intervention. After analyzing the stigma codes, we used the Health Stigma and Discrimination Framework to organize the data into four key domains: drivers, manifestations, outcomes, and health and social impacts.
Major drivers of HIV stigma included fear of HIV transmission, negative effects of antiretroviral therapy (ART), association with death, inaccurate knowledge, and negative attitudes towards ALWH. The most common manifestations of HIV stigma were gossip, insults and mocking, and physical and social distancing. Decreased ART adherence and missed HIV appointments were commonly cited outcomes of HIV stigma. Broader health impacts of HIV stigma were notable for mental health comorbidities including depression, anxiety, substance use, and suicidality. Identified resilience strategies included support for HIV care engagement and psychosocial support from family and friends.
This study systematically describes the stigmatization process faced by ALWH and experiencing depressive symptoms in Malawi. Notably, HIV stigma continues to disrupt HIV care and detrimentally impacts mental health during adolescent development. Further studies focused specifically on stigma are needed to better characterize this process and identify additional resilience factors. Investment in stigma-reduction interventions for ALWH is needed to avert poor mental health and HIV outcomes.
在马拉维,约25%的感染艾滋病毒的青少年(ALWH)也患有抑郁症。艾滋病毒污名不仅是导致抑郁症的主要因素,还对艾滋病毒护理参与产生不利影响。ALWH可能会将艾滋病毒污名体验为刻板印象、社会排斥、社会支持不足和虐待,而这些经历与心理健康不佳有关。尽管人们认识到艾滋病毒污名的有害影响,但我们对合并抑郁症的ALWH如何体验污名了解有限。在健康污名与歧视框架的指导下,我们描述了马拉维ALWH和合并抑郁症所面临的污名及其对未来干预措施的影响。
作为一项更大规模的适应性心理健康咨询干预形成性研究的一部分,我们对25名ALWH、4名ALWH的照顾者、3名艾滋病毒提供者以及之前一项心理健康咨询干预的5名参与者和5名工作人员进行了深入访谈、社会支持映射会议和焦点小组讨论。在分析污名编码后,我们使用健康污名与歧视框架将数据组织成四个关键领域:驱动因素、表现形式、后果以及健康和社会影响。
艾滋病毒污名的主要驱动因素包括对艾滋病毒传播的恐惧、抗逆转录病毒疗法(ART)的负面影响、与死亡的关联、知识不准确以及对ALWH的负面态度。艾滋病毒污名最常见的表现形式是流言蜚语、侮辱和嘲笑,以及身体和社交上的疏远。ART依从性降低和错过艾滋病毒预约是艾滋病毒污名常见的后果。艾滋病毒污名对更广泛健康的影响在包括抑郁症、焦虑症、物质使用和自杀倾向等心理健康合并症方面尤为明显。确定的复原力策略包括对艾滋病毒护理参与的支持以及来自家人和朋友的心理社会支持。
本研究系统地描述了马拉维ALWH以及经历抑郁症状者所面临的污名化过程。值得注意的是,艾滋病毒污名在青少年发育过程中继续扰乱艾滋病毒护理并对心理健康产生不利影响。需要开展专门针对污名的进一步研究,以更好地描述这一过程并确定其他复原力因素。需要对减少ALWH污名的干预措施进行投资,以避免不良的心理健康和艾滋病毒结局。