John Kristen M, Wenn Peter, Hai Ofek, Zeltser Roman, Makaryus Amgad N
Department of Cardiology, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY 11549, USA.
Division of Cardiology, HCA Brandon Regional Hospital, Brandon, FL 33511, USA.
J Clin Med. 2024 Nov 29;13(23):7279. doi: 10.3390/jcm13237279.
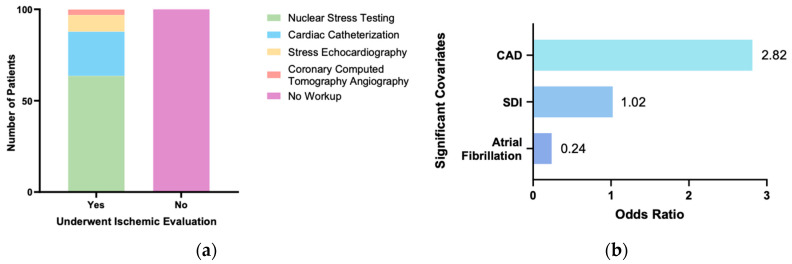
Coronary artery disease (CAD) is a common and treatable cause of heart failure (HF), but ischemic evaluation is often overlooked when evaluating patients with new-onset HF. Here, we sought to discern demographic and clinical predictors of ischemic workup in patients with newly diagnosed HF. A retrospective study of 200 consecutive patients with new-onset HF admitted to our safety-net hospital between 2011 and 2015 was performed. We developed a multivariate logistic regression model to analyze determinants of undergoing ischemic evaluation. A total of 99 patients (49.5%) underwent ischemic workup, while 101 patients (50.5%) did not. The mean age of the cohort was 73.9 ± 16, with 50% as male and 51% as White. In total, 41.5% of patients had HF with reduced ejection fraction, and 37% of patients had HF with preserved ejection fraction. Among the patients who underwent ischemic evaluation, 63.6% received nuclear stress testing, 24.2% received cardiac catheterization, 9.1% received stress echocardiography, and 3% received computed tomography angiography. Demographic and clinical factors such as sex, age, race, presence of hypertension, hyperlipidemia, chronic kidney disease, diabetes, or obesity had no significant association with receiving ischemic workup ( > 0.05). Patients with known CAD (OR 2.816, = 0.015) and a higher social deprivation index (SDI) (OR 1.022, = 0.003) were significantly more likely to receive an ischemic evaluation. Atrial fibrillation was significantly negatively associated with receiving ischemic workup (OR: 0.24; = 0.001). In our single-center safety-net hospital analysis, known CAD and higher SDI were significant predictors of ischemic evaluation in patients with newly diagnosed HF. Multiple demographic features, including age, sex, race, and clinical features, including HF type, hypertension, hyperlipidemia, and diabetes, had no significant correlation with ischemic workup.
冠状动脉疾病(CAD)是心力衰竭(HF)常见且可治疗的病因,但在评估新发HF患者时,缺血性评估常常被忽视。在此,我们试图识别新诊断HF患者进行缺血性检查的人口统计学和临床预测因素。对2011年至2015年间入住我们安全网医院的200例连续新发HF患者进行了一项回顾性研究。我们建立了一个多因素逻辑回归模型来分析接受缺血性评估的决定因素。共有99例患者(49.5%)接受了缺血性检查,而101例患者(50.5%)未接受。该队列的平均年龄为73.9±16岁,50%为男性,51%为白人。总体而言,41.5%的患者射血分数降低的HF,37%的患者射血分数保留的HF。在接受缺血性评估的患者中,63.6%接受了核素负荷试验,24.2%接受了心导管检查,9.1%接受了负荷超声心动图检查,3%接受了计算机断层血管造影。性别、年龄、种族、高血压、高脂血症、慢性肾病、糖尿病或肥胖等人口统计学和临床因素与接受缺血性检查无显著相关性(>0.05)。已知CAD的患者(OR 2.816, = 0.015)和较高的社会剥夺指数(SDI)(OR 1.022, = 0.003)接受缺血性评估的可能性显著更高。心房颤动与接受缺血性检查显著负相关(OR:
0.24; = 0.001)。在我们的单中心安全网医院分析中,已知CAD和较高的SDI是新诊断HF患者进行缺血性评估的显著预测因素。包括年龄、性别、种族在内的多种人口统计学特征以及包括HF类型、高血压、高脂血症和糖尿病在内的临床特征与缺血性检查无显著相关性。