Miller Daniel L, Hutchins Jacob, Ferguson Michael A, Barhoush Yazid, Achter Emily, Kuckelman John P
Medical College Georgia, 1120 15th Street, BA 4300, Augusta, GA, USA.
University Minnesota, Minneapolis, MN, USA.
Pain Ther. 2025 Feb;14(1):317-328. doi: 10.1007/s40122-024-00694-3. Epub 2024 Dec 17.
The cost benefit of intercostal nerve cryoablation during surgical lobectomy for postoperative pain management is unknown. The current study compared hospital economics, resource use, and clinical outcomes during the index stay and accompanying short-term follow-up. Patients who underwent lobectomy with standard of care treatment for postsurgical pain management and cryoablation were compared to those with standard of care treatment only. We hypothesized that cryoablation would reduce narcotic use and index hospital and short-term costs.
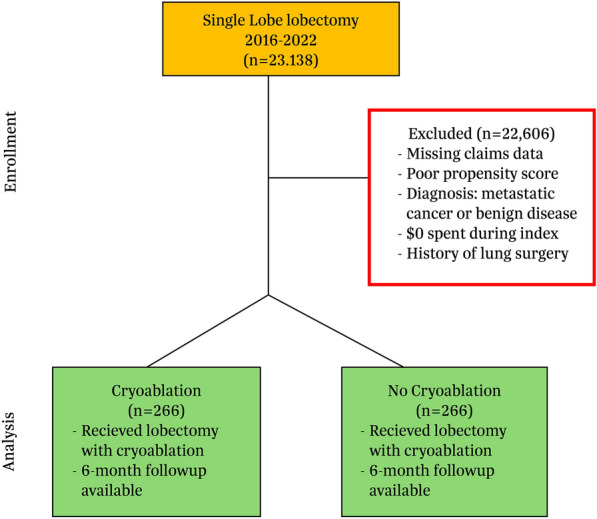
A retrospective, propensity matched cohort of surgical patients treated between 2016 and 2022 from a US National All-Payer Database were used. Cost and outcome comparisons were made between groups using chi-square and t tests.
From a cohort of 23,138 patients, 266 pairs with a mean age of 69 years were included. Matching variables included age, gender, lobe resected, and prior opioid use. Both groups had significant comorbidity history and prior opioid use; 66% (n = 175 both groups) underwent open lobectomy and 53% (n = 142 vs. 143) had the upper lobe resected. Cryoablation intervention was associated with 1.3 days reduced hospital stay (8.8 vs. 10.1 days, p = 0.31) and no difference in perioperative safety. After 90 days, postsurgery cryoablation patients had lower opioid prescription refills (27.3 vs. 36.9 morphine milligram equivalents, p = 0.03). Cryoablation patient costs trended less than non-cryoablation patients during index ($38,753 vs. $43,974, p = 0.10) and lower through 6 months (total costs, $65,703 vs. $74,304, p = 0.10). There was no difference in postsurgery resource use, but a smaller proportion of cryoablation patients had outpatient hospital visits (83.1%, N = 221 vs. 92.9%, n = 247, p < 0.01).
Cryoablation during lobectomy is safe and does not add incremental hospital costs. Clinical meaningful reductions in length of stay and postsurgery opioid use were observed with cryoablation intervention. The addition of cryoablation during surgery to reduce postoperative pain appears to be a cost-effective therapy.
在肺叶切除术中进行肋间神经冷冻消融术以管理术后疼痛的成本效益尚不清楚。本研究比较了在首次住院期间及随后的短期随访中的医院经济学、资源利用和临床结果。将接受肺叶切除术并采用标准护理治疗术后疼痛管理和冷冻消融术的患者与仅采用标准护理治疗的患者进行比较。我们假设冷冻消融术将减少麻醉药物的使用以及首次住院和短期费用。
使用来自美国国家全支付者数据库的2016年至2022年期间接受治疗的手术患者的回顾性倾向匹配队列。使用卡方检验和t检验对组间的成本和结果进行比较。
在23138名患者队列中,纳入了266对平均年龄为69岁的患者。匹配变量包括年龄、性别、切除的肺叶和先前的阿片类药物使用情况。两组均有显著的合并症病史和先前的阿片类药物使用情况;66%(两组均为n = 175)接受了开放性肺叶切除术,53%(n = 142对143)切除了上叶。冷冻消融干预与住院时间缩短1.3天相关(8.8天对10.1天,p = 0.31),围手术期安全性无差异。90天后,术后接受冷冻消融术的患者阿片类药物处方续用量较低(27.3对36.9吗啡毫克当量,p = 0.03)。在首次住院期间,冷冻消融术患者的费用趋势低于非冷冻消融术患者(38753美元对43974美元,p = 0.10),在6个月内费用更低(总成本,65703美元对74304美元,p = 0.10)。术后资源利用情况无差异,但冷冻消融术患者门诊就诊的比例较小(83.1%,N = 221对92.9%,n = 247,p < 0.01)。
肺叶切除术中的冷冻消融术是安全的,不会增加额外的住院费用。冷冻消融干预观察到住院时间和术后阿片类药物使用有临床意义的减少。在手术中增加冷冻消融术以减轻术后疼痛似乎是一种具有成本效益的治疗方法。