Liang Lei, Xu Ning, Ding Lanfei, Li Xin, Jiang Chengxun, Zhang Jianhua, Yang Jun
Department of Surgical Oncology, The First Affiliated Hospital of Kunming Medical University, Kunming, 650032, China.
Department of Emergency, The Second People's Hospital of Honghe Prefecture, Jianshui, 654300, China.
BMC Cancer. 2024 Dec 18;24(1):1548. doi: 10.1186/s12885-024-13331-1.
Inflammation-related biomarkers, such as systemic inflammation score (SIS) and neutrophil-lymphocyte ratio (NLR), are associated with colorectal cancer prognosis. However, the combined role of SIS, NLR, and clinicopathological factors in stage II/III colorectal cancer remains unclear. This study developed a nomogram to predict long-term prognosis for these patients.
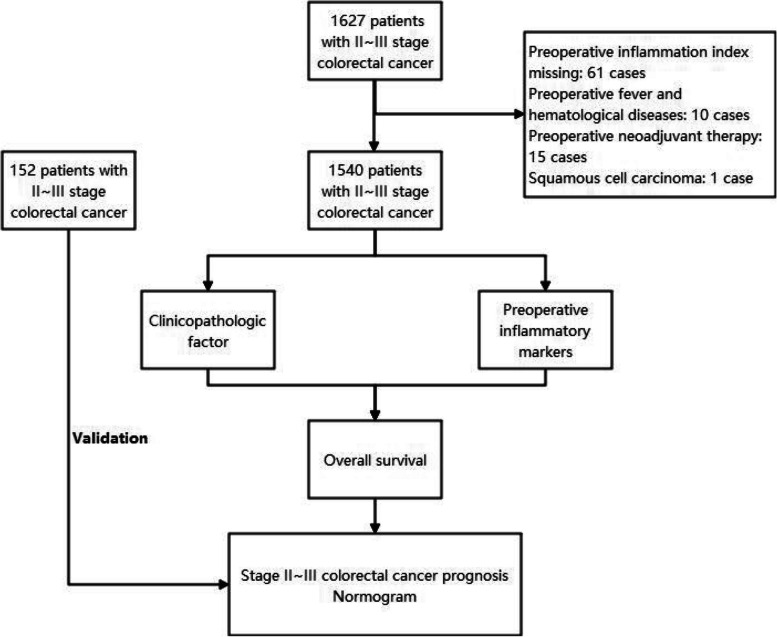
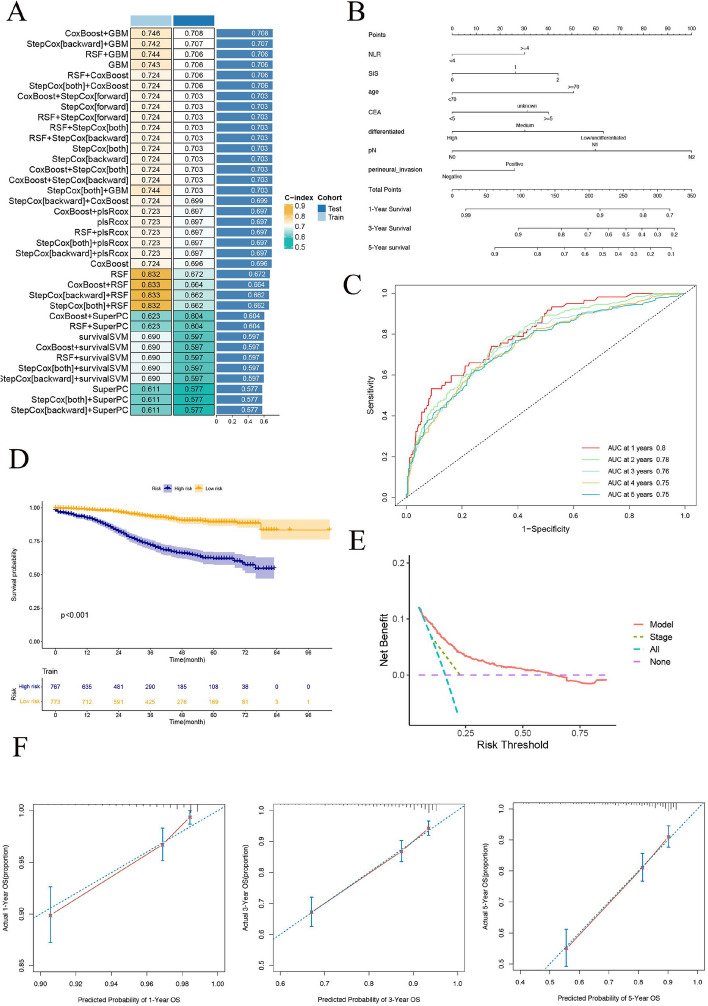
This retrospective study included 1540 patients (training set) from the First Affiliated Hospital of Kunming Medical University and 152 patients (testing set) from The Honghe Third People's Hospital. Cox regression identified independent prognostic factors, and machine learning established predictive models. Model performance was evaluated by the C-index, area under the curve (AUC), and decision curve analysis (DCA).
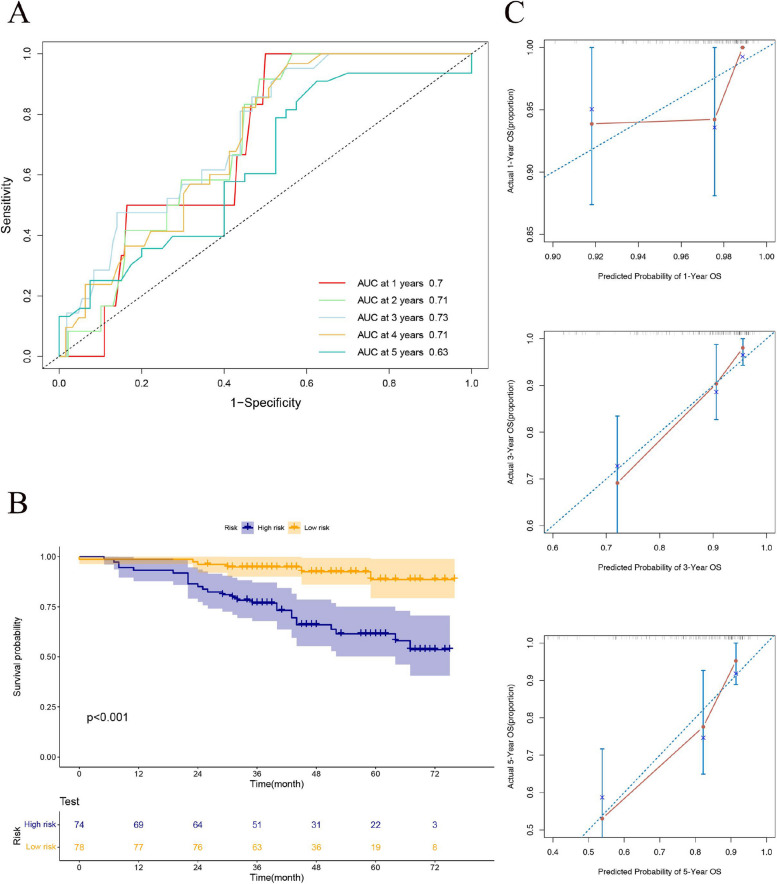
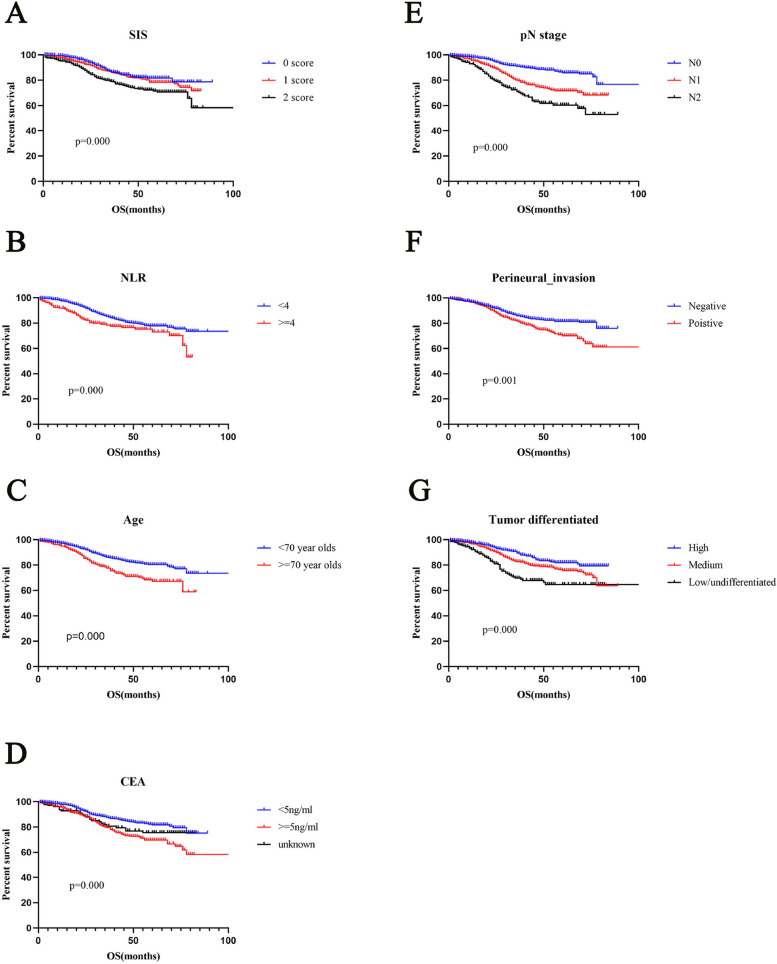
In the training set, a total of 1540 patients with stage II/III colorectal cancer were included. More than 70 years old (HR = 1.830, p = 0.000); SIS = 2 (HR = 1.693, p = 0.002); Preoperative CEA more than 5 ng/mL (HR = 1.614, p = 0.000); and Moderately differentiated (HR = 1.438, p = 0.011); or Low/undifferentiated (HR = 2.126, p = 0.000); The pN1 (HR = 2.040, p = 0.000) and pN2 (HR = 3.297, p = 0.000) stages were considered independent prognostic risk factors of stage II/III colorectal cancer. Negative perineural invasion (HR = 0.733, p = 0.014) and NLR less than 4 (HR = 0.696, p = 0.022) were considered independent prognostic protective factors of stage II/III colorectal cancer. A nomogram was established based on SIS, NLR, and the clinicopathological results for predicting and validating the overall survival in the training and testing sets. The C-index of the training set was 0.746, and the C-index of the testing set was 0.708, indicating the high prediction efficiency of the nomogram.
A nomogram combining SIS, NLR, and clinicopathological factors provides an effective, cost-efficient tool for predicting the prognosis of stage II/III colorectal cancer. Future studies will validate its long-term predictive performance in larger, multicenter cohorts.
炎症相关生物标志物,如全身炎症评分(SIS)和中性粒细胞与淋巴细胞比值(NLR),与结直肠癌预后相关。然而,SIS、NLR及临床病理因素在Ⅱ/Ⅲ期结直肠癌中的联合作用仍不清楚。本研究开发了一种列线图来预测这些患者的长期预后。
这项回顾性研究纳入了昆明医科大学第一附属医院的1540例患者(训练集)和红河州第三人民医院的152例患者(测试集)。Cox回归确定独立预后因素,机器学习建立预测模型。通过C指数、曲线下面积(AUC)和决策曲线分析(DCA)评估模型性能。
在训练集中,共纳入1540例Ⅱ/Ⅲ期结直肠癌患者。年龄大于70岁(HR = 1.830,p = 0.000);SIS = 2(HR = 1.693,p = 0.002);术前癌胚抗原大于5 ng/mL(HR = 1.614,p = 0.000);中度分化(HR = 1.438,p = 0.011)或低分化/未分化(HR = 2.126,p = 0.000);pN1(HR = 2.040,p = 0.000)和pN2(HR = 3.297,p = 0.000)期被认为是Ⅱ/Ⅲ期结直肠癌的独立预后危险因素。神经周围浸润阴性(HR = 0.733,p = 0.014)和NLR小于4(HR = 0.696,p = 0.022)被认为是Ⅱ/Ⅲ期结直肠癌的独立预后保护因素。基于SIS、NLR及临床病理结果建立列线图,用于预测和验证训练集和测试集中的总生存期。训练集的C指数为0.746,测试集的C指数为0.708,表明列线图具有较高的预测效率。
结合SIS、NLR及临床病理因素的列线图为预测Ⅱ/Ⅲ期结直肠癌的预后提供了一种有效且经济高效的工具。未来的研究将在更大规模的多中心队列中验证其长期预测性能。