Jang Chul-Young, Kang Kyoung-Tak, Hong Hyongtaek, Jung Min, Kim Sungjun, Yoo Je-Hyun, Kim Sung-Hwan
Department of Orthopedic Surgery, Yonsei University College of Medicine, Seoul, Republic of Korea.
Department of Mechanical Engineering, Yonsei University, 50 Yonsei-ro, Seodaemun-gu, Seoul, Republic of Korea.
J Orthop Surg Res. 2024 Dec 19;19(1):850. doi: 10.1186/s13018-024-05373-9.
No clear agreement exists on the degree of bone formation required to remove a metal plate without correction loss after medial opening-wedge high tibial osteotomy (MOWHTO). We aimed to investigate the mechanical stability of the proximal tibia with different bone formations after plate removal in MOWHTO using finite element models and determine the extent of bone formation when the plate can be removed without correction loss.
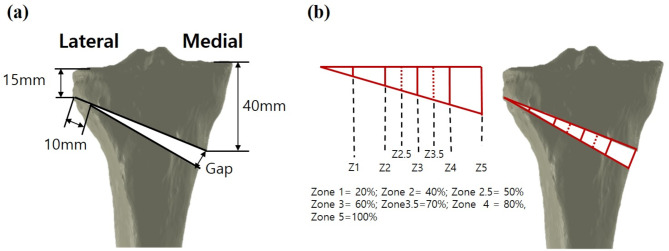
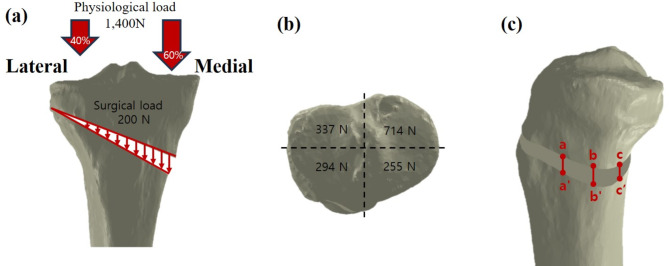
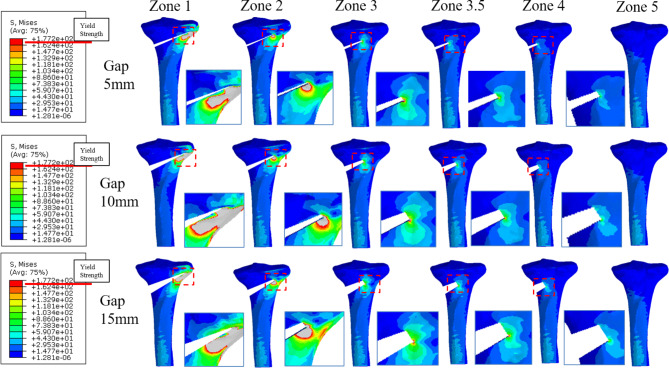
The MOWHTO models with 5, 10, and 15 mm opening gaps were generated. The mechanical stability of proximal tibial models with different extents of bone formation (from the lateral cortex of the osteotomy wedge to 20% (zone 1), 40% (zone 2), 50% (zone 2.5), 60% (zone 3), 70% (zone 3.5), 80% (zone 4), and 100% bone formation medially) after plate removal was analyzed using finite element analysis. Bone stress and strain and micromotion were evaluated to investigate fracture risk and bone stability, respectively, in various types of tibial models.
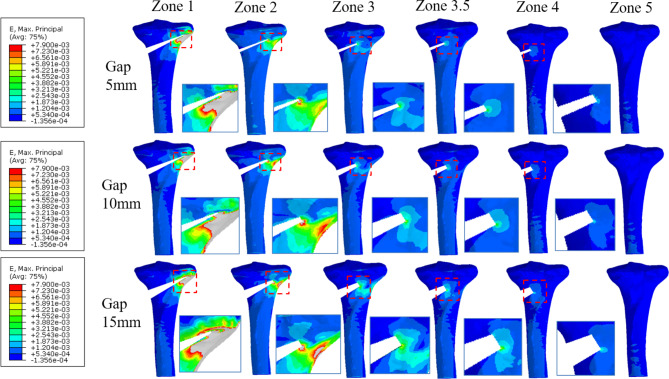
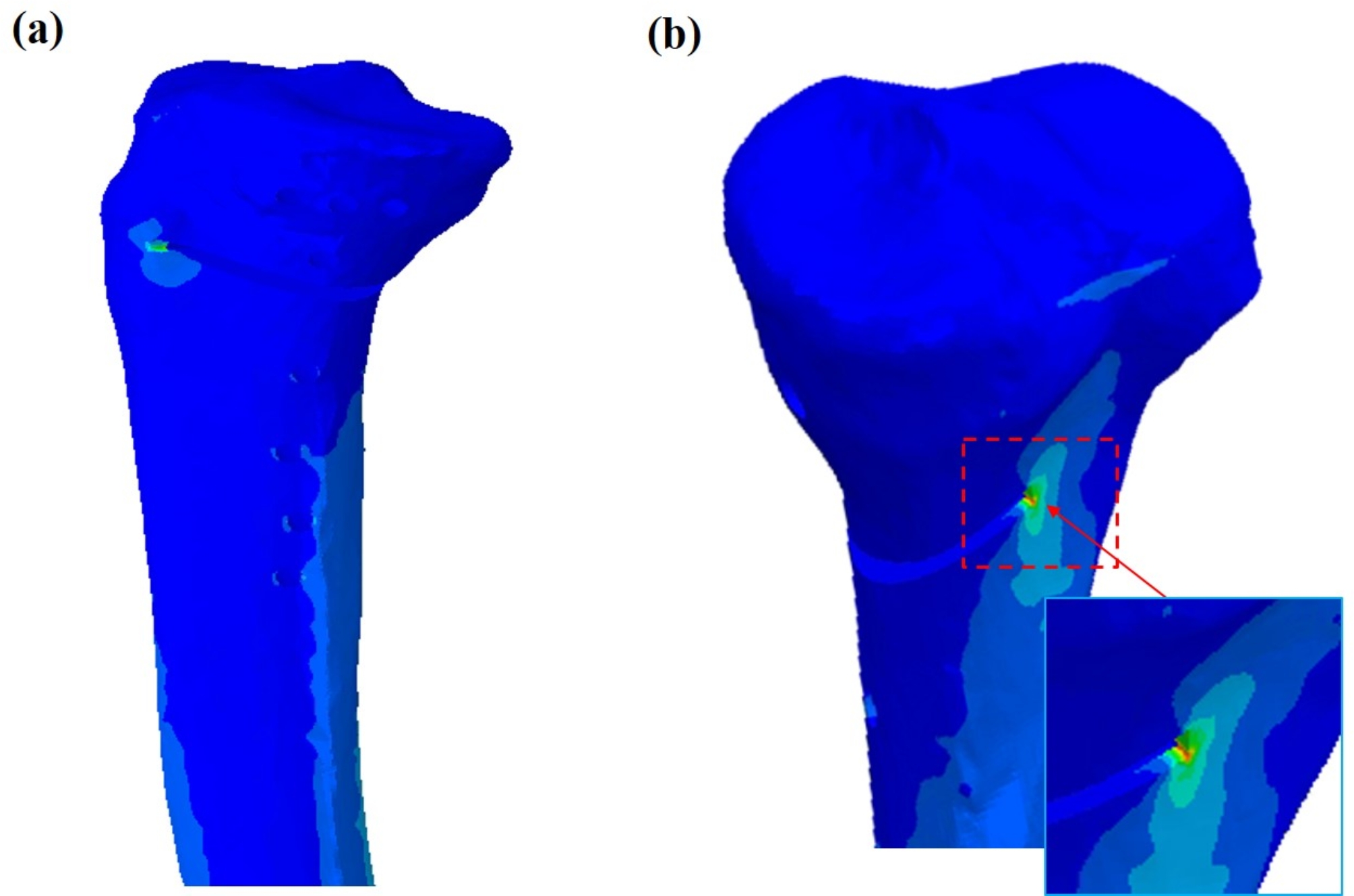
Peak von Mises stress was lower than yield strength when bone formation reached zone 3.5 (70%) or more in 5- and 10-mm osteotomy gap models, and zone 4 (80%) or more in a 15-mm gap model. Maximal principal strains were lower than 6,130 microstrain when bone formation reaches zone 3.5 (70%) or more in models with osteotomy gaps of 5, 10, and 15 mm.
This indicates that plate removal without correction loss after MOWHTO may be possible when bone formation reaches zone 3.5 (> 70%) or more during 5- and 10-mm osteotomy gap corrections, and zone 4 (> 80%) or more during 15-mm gap correction. The present study results suggest that it would be safer to perform plate removal after obtaining sufficient bone formation rather than performing it near the osteotomy gap center (50%) to avoid correction loss considering both coronal and sagittal plane aspects.
对于内侧开放楔形高位胫骨截骨术(MOWHTO)后,在不发生矫正丢失的情况下取出金属板所需的骨形成程度,目前尚无明确共识。我们旨在使用有限元模型研究MOWHTO术后不同骨形成情况下胫骨近端的力学稳定性,并确定在不发生矫正丢失的情况下可以取出钢板时的骨形成范围。
建立截骨间隙分别为5、10和15mm的MOWHTO模型。使用有限元分析评估取出钢板后不同骨形成程度(从截骨楔形外侧皮质到内侧骨形成20%(区域1)、40%(区域2)、50%(区域2.5)、60%(区域3)、70%(区域3.5)、80%(区域4)和100%)的胫骨近端模型的力学稳定性。分别评估各种类型胫骨模型的骨应力、应变和微动,以研究骨折风险和骨稳定性。
在截骨间隙为5mm和10mm的模型中,当骨形成达到区域3.5(70%)或更高时,von Mises应力峰值低于屈服强度;在截骨间隙为15mm的模型中,当骨形成达到区域4(80%)或更高时,von Mises应力峰值低于屈服强度。在截骨间隙为5mm、10mm和15mm的模型中,当骨形成达到区域3.5(70%)或更高时,最大主应变低于6130微应变。
这表明,在5mm和10mm截骨间隙矫正过程中,当骨形成达到区域3.5(>70%)或更高时,以及在15mm截骨间隙矫正过程中,当骨形成达到区域4(>80%)或更高时,MOWHTO术后可能可以在不发生矫正丢失的情况下取出钢板。本研究结果表明,考虑到冠状面和矢状面,在获得足够的骨形成后取出钢板比在截骨间隙中心(50%)附近取出钢板更安全,以避免矫正丢失。