Syed Izna Najam, Syed Noem Najam, Naseem Rabail, Singh-Ranger Deepak
General Surgery, The Royal Wolverhampton NHS Trust, Wolverhampton, GBR.
General Surgery, Dr. Ruth K. M. Pfau Civil Hospital Karachi, Karachi, PAK.
Cureus. 2024 Nov 20;16(11):e74073. doi: 10.7759/cureus.74073. eCollection 2024 Nov.
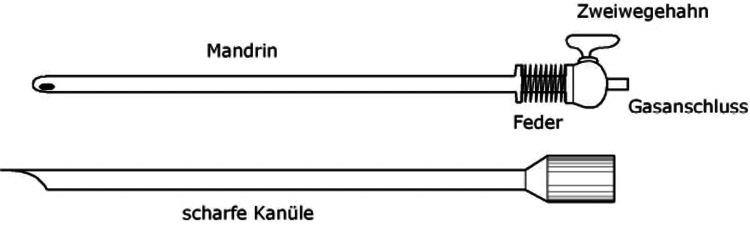
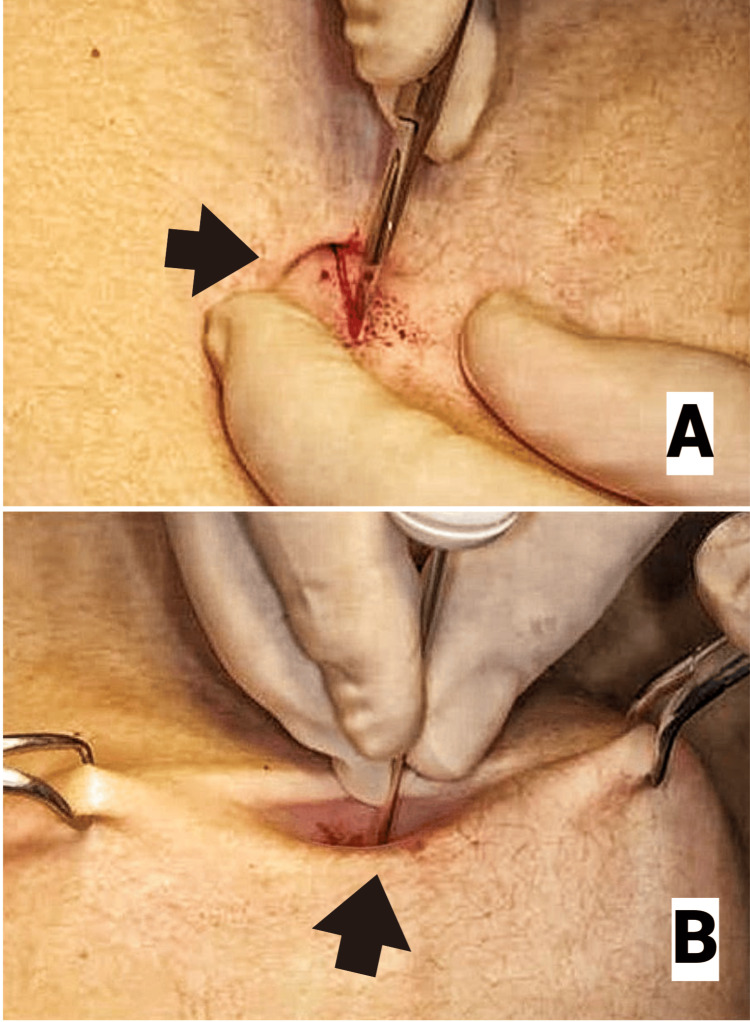
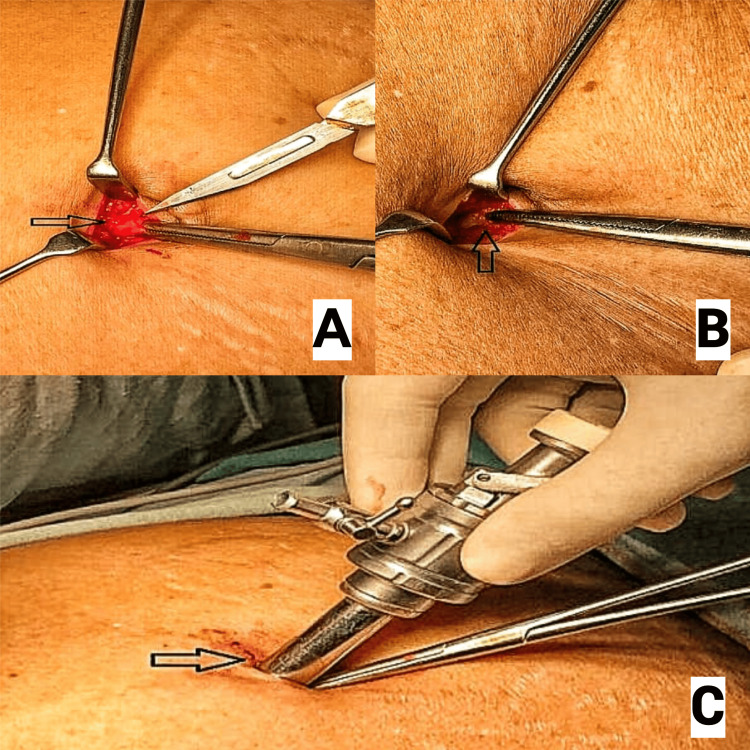
Classically, there are two techniques for establishing pneumoperitoneum in laparoscopic and robotic surgeries: the closed Veress needle technique and Hasson's technique for open placement of laparoscopic ports. Most surgeons prefer the open Hasson technique, even though it is not the gold standard. Some surgeons still favour the Veress needle technique despite literature linking it to visceral and vascular damage.
This study aimed at determining the safety index of the two techniques of establishing pneumoperitoneum in laparoscopic and robotic surgeries by evaluating the risk of injuries associated with Veress and Hasson's techniques.
This is a retrospective cohort study evaluating the incidence of primary port placement injuries (PPPI) using Hasson's open trocar technique and Veress needle technique in 200 laparoscopic and robotic cases (emergency vs. elective) over a three-month period (January to March 2024) at Newcross Hospital. The exclusion criteria were secondary port injuries. IBM SPSS Statistics for Windows, Version 24 (Released 2016; IBM Corp., Armonk, New York) and Microsoft Excel (Microsoft Corporation, Redmond, Washington) were used for data analysis.
Hasson's open technique of primary port placement was used in 74% of emergency cases, while the Veress needle technique was used in 26% of emergency surgeries. Similarly, the most common technique for establishing pneumoperitoneum employed in elective surgical procedures was Hasson's open technique (77%). When comparing the safety index of the two techniques for establishing pneumoperitoneum, we found that there were no major PPPI associated with either technique, with minimal incidence of minor PPPI associated with both techniques. While some cases did involve injuries from secondary port insertions (bowel and vascular injuries), these were excluded according to our exclusion criteria. Additionally, no perioperative mortality associated with primary trocar placement was observed.
Although the literature describes the association of the Veress technique with visceral and vascular injuries, our study found it to be as safe as Hasson's open port placement technique. Therefore, either technique can be employed for the safe establishment of pneumoperitoneum in laparoscopic and robotic surgeries.
传统上,在腹腔镜手术和机器人手术中建立气腹有两种技术:闭合式Veress针技术和用于开放式放置腹腔镜端口的哈森技术。大多数外科医生更喜欢开放式哈森技术,尽管它并非金标准。尽管有文献将Veress针技术与内脏和血管损伤联系起来,但一些外科医生仍然青睐该技术。
本研究旨在通过评估与Veress技术和哈森技术相关的损伤风险,确定腹腔镜手术和机器人手术中两种建立气腹技术的安全指数。
这是一项回顾性队列研究,在纽克罗斯医院对200例腹腔镜手术和机器人手术病例(急诊与择期)进行为期三个月(2024年1月至3月)的研究,评估使用哈森开放式套管针技术和Veress针技术时原发性端口置入损伤(PPPI)的发生率。排除标准为继发性端口损伤。使用IBM SPSS Statistics for Windows 24版(2016年发布;IBM公司,纽约州阿蒙克)和Microsoft Excel(微软公司,华盛顿州雷德蒙德)进行数据分析。
在74%的急诊病例中使用了哈森开放式原发性端口置入技术,而在26%的急诊手术中使用了Veress针技术。同样,择期手术中建立气腹最常用的技术是哈森开放式技术(77%)。在比较两种建立气腹技术的安全指数时,我们发现两种技术均未出现重大PPPI,两种技术的轻微PPPI发生率均极低。虽然有些病例确实涉及继发性端口插入造成的损伤(肠道和血管损伤),但根据我们的排除标准将这些病例排除。此外,未观察到与原发性套管针置入相关的围手术期死亡。
尽管文献描述了Veress技术与内脏和血管损伤的关联,但我们的研究发现它与哈森开放式端口置入技术一样安全。因此,在腹腔镜手术和机器人手术中,两种技术均可用于安全建立气腹。