Gupta Amulya, Sattar Zeeshan, Chaaban Nourhan, Ranka Sagar, Carlson Cameron, Sami Farhad, Robinson Clifford G, Cuculich Phillip S, Sheldon Seth H, Reddy Madhu, Akhavan David, Noheria Amit
Department of Cardiovascular Medicine, The University of Kansas Medical Center, 3901 Rainbow Blvd., Mail Stop 4023, Kansas City, KS 66160, USA.
Department of General and Hospital Medicine, The University of Kansas Medical Center, Kansas City, KS, USA.
Europace. 2024 Dec 26;27(1). doi: 10.1093/europace/euae305.
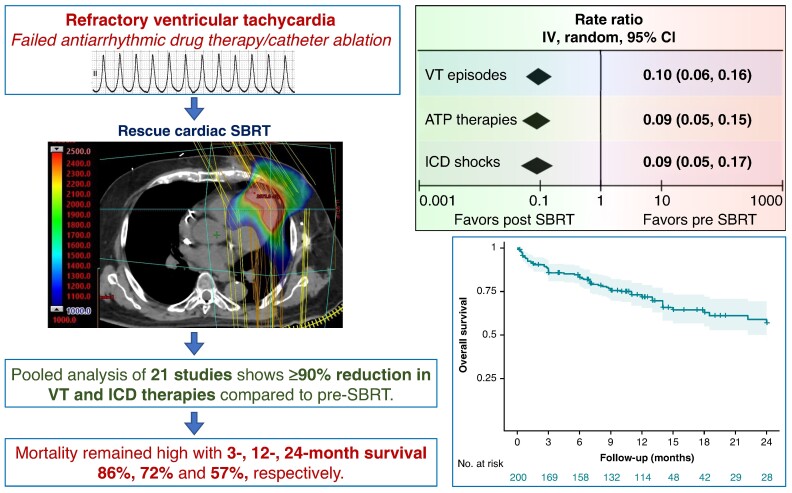
Among patients with structural heart disease with ventricular tachycardia (VT) refractory to medical therapy and catheter ablation, cardiac stereotactic body radiotherapy (SBRT) is a paradigm-changing treatment option. This study aims to assess the efficacy of cardiac SBRT in refractory VT by comparing the rates of VT episodes, anti-tachycardia pacing (ATP) therapies, and implantable cardioverter-defibrillator (ICD) shocks post-SBRT with pre-SBRT.
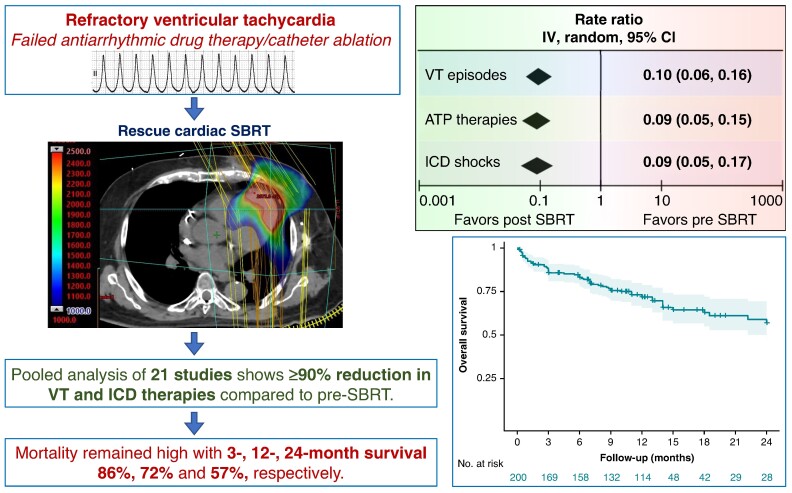
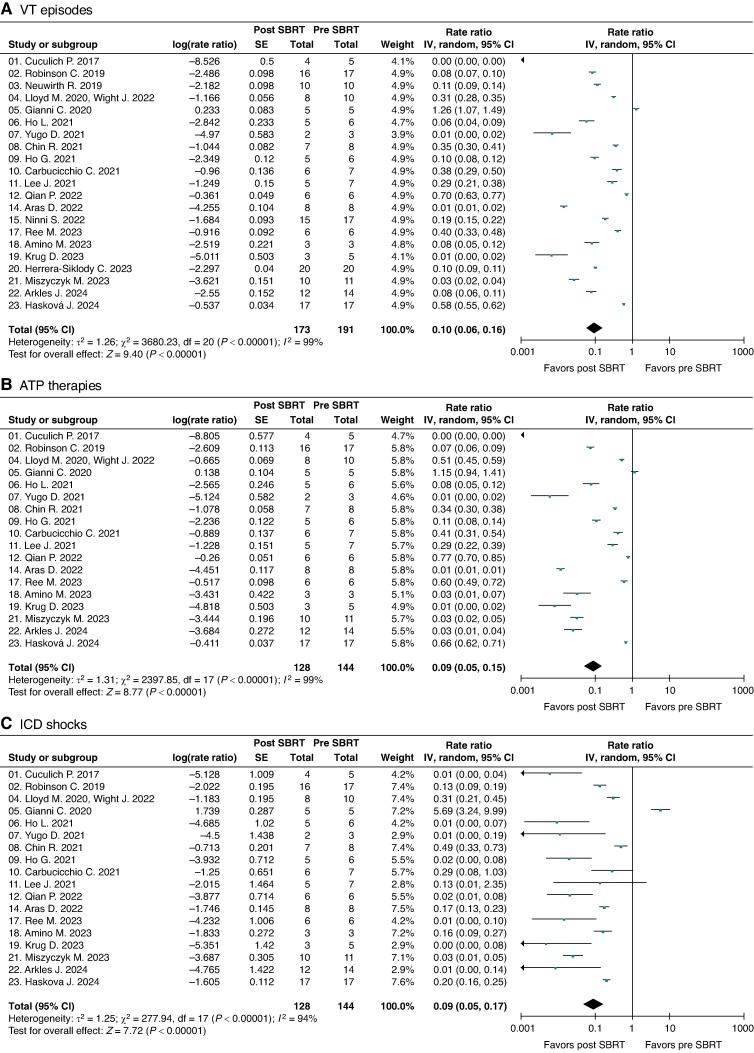
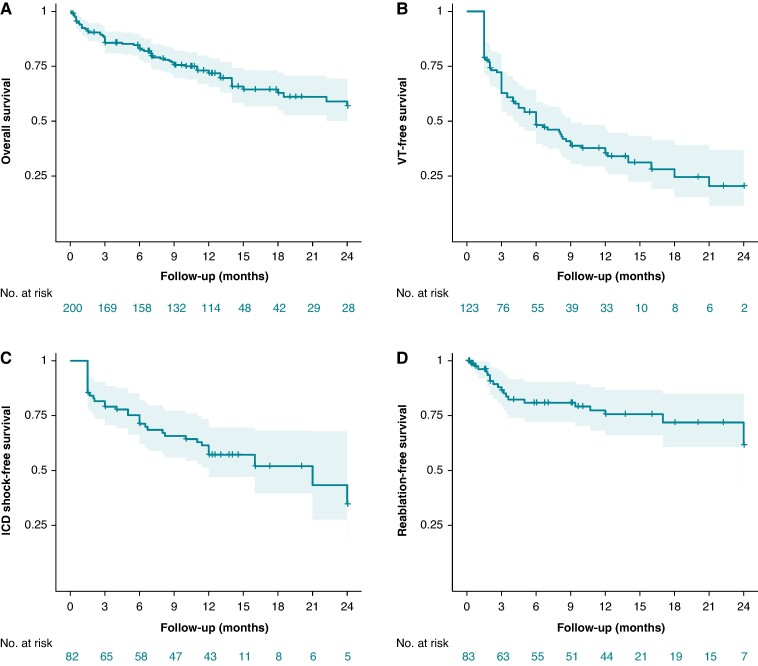
We performed a comprehensive literature search and included all clinical studies reporting outcomes on cardiac SBRT for VT. Treatment efficacy was evaluated as random-effects pooled rate-ratios of VT episodes, ATP therapies and ICD shocks post-SBRT (after 6-week blanking) and pre-SBRT, with patients serving as their own controls. Post-SBRT overall survival was assessed using Kaplan-Meier method. We included 23 studies published 2017-24 reporting on 225 patients who received cardiac SBRT, with median follow-up 5.8-28 months. There was significant heterogeneity among the studies for all three efficacy endpoints (P < 0.00001). The random-effects pooled rate-ratios of VT episodes, ATP therapies and ICD shocks post- vs. pre-SBRT were 0.10 (95% CI 0.06, 0.16), 0.09 (0.05, 0.15), and 0.09 (0.05, 0.17), respectively (all P < 0.00001). The most common reported complications included pericardial (8.0%, including 0.9% late oesophagogastro-pericardial fistula) and pulmonary (5.8%). There was no change in left ventricular ejection fraction post-SBRT (P = 0.3) but some studies reported an increase in mitral regurgitation. The combined 3-, 12-, and 24-month overall patient survival was 0.86 (0.80, 0.90), 0.72 (0.65, 0.78), and 0.57 (0.47, 0.67), respectively.
Among patients with refractory VT in context of structural heart disease, VT burden and ICD shocks are dramatically reduced following cardiac SBRT. The overall mortality in this population with heart failure and refractory VT receiving palliative cardiac SBRT remains high.
对于患有结构性心脏病且室性心动过速(VT)对药物治疗和导管消融难治的患者,心脏立体定向体部放疗(SBRT)是一种改变治疗模式的选择。本研究旨在通过比较SBRT后与SBRT前的VT发作率、抗心动过速起搏(ATP)治疗次数和植入式心律转复除颤器(ICD)电击次数,评估心脏SBRT对难治性VT的疗效。
我们进行了全面的文献检索,纳入了所有报告心脏SBRT治疗VT结果的临床研究。治疗效果评估为SBRT后(6周空白期后)与SBRT前VT发作、ATP治疗和ICD电击的随机效应合并率比,患者自身作为对照。使用Kaplan-Meier方法评估SBRT后的总生存率。我们纳入了2017年至2024年发表的23项研究,报告了225例接受心脏SBRT的患者,中位随访时间为5.8至28个月。所有三个疗效终点的研究之间均存在显著异质性(P < 0.00001)。SBRT后与SBRT前VT发作、ATP治疗和ICD电击的随机效应合并率比分别为0.10(95%CI为0.06,0.16)、0.09(0.05,0.15)和0.09(0.05,0.17)(均P < 0.00001)。报告的最常见并发症包括心包(8.0%,包括0.9%的晚期食管胃心包瘘)和肺部(5.8%)。SBRT后左心室射血分数无变化(P = 0.3),但一些研究报告二尖瓣反流增加。患者3个月、12个月和24个月的总生存率分别为0.86(0.80,0.90)、0.72(0.65,0.78)和0.57(0.47,0.67)。
在患有结构性心脏病的难治性VT患者中,心脏SBRT后VT负担和ICD电击次数显著减少。在接受姑息性心脏SBRT的心力衰竭和难治性VT患者中,总体死亡率仍然很高。