Kals Mart, Wilson Lindsay, Levey Daniel F, Parodi Livia, Steyerberg Ewout W, Richardson Sylvia, He Feng, Sun Xiaoying, Jain Sonia, Palotie Aarno, Ripatti Samuli, Rosand Jonathan, Manley Geoff T, Maas Andrew I R, Stein Murray B, Menon David K
Estonian Genome Center, Institute of Genomics, University of Tartu, Tartu, Estonia.
Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom.
EClinicalMedicine. 2024 Dec 5;78:102956. doi: 10.1016/j.eclinm.2024.102956. eCollection 2024 Dec.
Post-traumatic stress disorder (PTSD) and depression are common after mild traumatic brain injury (mTBI), but their biological drivers are uncertain. We therefore explored whether polygenic risk scores (PRS) derived for PTSD and major depressive disorder (MDD) are associated with the development of cognate TBI-related phenotypes.
Meta-analyses were conducted using data from two multicenter, prospective observational cohort studies of patients with mTBI: the CENTER-TBI study (ClinicalTrials.gov ID NCT02210221) in Europe (December 2014-December 2017) and the TRACK-TBI study in the US (March 2014-July 2018). In both cohorts, the most common causes of injury were road traffic accidents and falls. Primary outcomes, specifically probable PTSD and depression, were defined at 6 months post-injury using scores ≥33 on the PTSD Checklist-5 and ≥15 on the Patient Health Questionnaire-9, respectively. We calculated PTSD-PRS and MDD-PRS for patients aged ≥17 years who had a Glasgow Coma Scale score of 13-15 upon hospital arrival and assessed their association with PTSD and depression following TBI. We also evaluated the transferability of the findings in a cohort of African Americans.
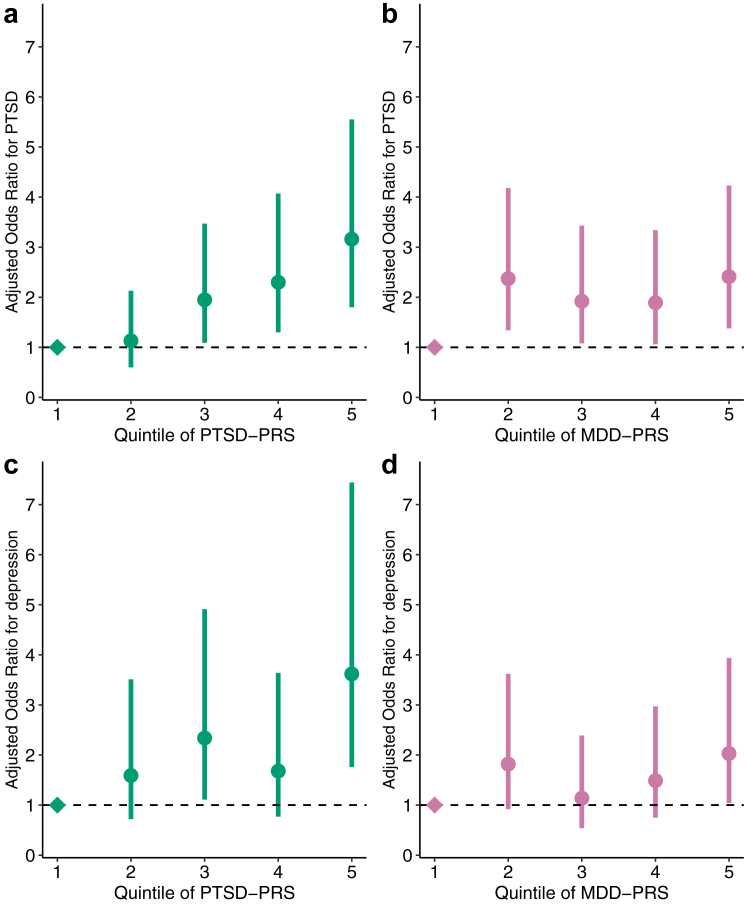
Overall, 11.8% (219/1869) and 6.7% (124/1869) patients were classified as having probable PTSD and depression, respectively. The PTSD-PRS was significantly associated with higher adjusted odds of PTSD in both cohorts, with a pooled odds ratio (OR) of 1.55 [95% confidence interval (CI) 1.30-1.84, < 0.001, = 20.8%]. Although the MDD-PRS increased the risk of depression after TBI, it did not reach significance in the individual cohorts. However, in a combined analysis, the risk was significantly elevated with a pooled OR of 1.26 [95% CI 1.03-1.53, = 0.02, = 0%]. The addition of PRSs improved the proportion of outcome variance explained in the two study cohorts from 19.5% and 30.3% to 21.6% and 34.0% for PTSD; and from 11.0% and 22.5% to 12.8% and 22.6% for depression. Patients in the highest cognate PRS quintile had increased odds of 3.16 [95% CI 1.80-5.55] and 2.03 [95% CI 1.04-3.94] of developing PTSD or depression compared to the lowest quintile, respectively.
Associations of PRSs with PTSD and depression following TBI are not disorder-specific. However, the overlap between MDD-PRS and depression following TBI is less robust compared to PTSD-PRS and PTSD. PRSs could improve risk prediction, and permit enrichment for interventional trials.
This study was supported by funding by an FP7 grant from the European Union, Hannelore Kohl Stiftung, Integra LifeSciences Corporation, NeuroTrauma Sciences, US National Institutes of Health, US Department of Defense, National Football League Advisory Board, US Department of Energy, and One Mind.
创伤后应激障碍(PTSD)和抑郁症在轻度创伤性脑损伤(mTBI)后很常见,但其生物学驱动因素尚不确定。因此,我们探讨了针对PTSD和重度抑郁症(MDD)得出的多基因风险评分(PRS)是否与同源TBI相关表型的发展有关。
使用来自两项针对mTBI患者的多中心前瞻性观察队列研究的数据进行荟萃分析:欧洲的CENTER-TBI研究(ClinicalTrials.gov标识符NCT02210221)(2014年12月至2017年12月)和美国的TRACK-TBI研究(2014年3月至2018年7月)。在这两个队列中,最常见的受伤原因是道路交通事故和跌倒。主要结局,即具体的可能的PTSD和抑郁症,分别在受伤后6个月使用PTSD检查表-5得分≥33和患者健康问卷-9得分≥15来定义。我们计算了入院时格拉斯哥昏迷量表评分为13-15分的≥17岁患者的PTSD-PRS和MDD-PRS,并评估了它们与TBI后PTSD和抑郁症的关联。我们还在一组非裔美国人队列中评估了研究结果的可转移性。
总体而言,分别有11.8%(219/1869)和6.7%(124/1869)的患者被分类为可能患有PTSD和抑郁症。PTSD-PRS与两个队列中PTSD的更高调整后比值显著相关,合并比值比(OR)为1.55[95%置信区间(CI)1.30-1.84,<0.001,解释变异百分比=20.8%]。虽然MDD-PRS增加了TBI后患抑郁症的风险,但在各个队列中未达到显著水平。然而,在综合分析中,风险显著升高,合并OR为1.26[95%CI 1.03-1.53,P=0.02,解释变异百分比=0%]。添加PRS后,两个研究队列中PTSD结局变异的解释比例从19.5%和30.3%提高到21.6%和34.0%;抑郁症的解释比例从11.0%和22.5%提高到12.8%和22.6%。与最低五分位数相比,同源PRS最高五分位数的患者患PTSD或抑郁症的几率分别增加了3.16[95%CI 1.80-5.55]和2.03[95%CI 1.04-3.94]。
PRS与TBI后PTSD和抑郁症的关联并非疾病特异性。然而,与PTSD-PRS和PTSD相比,MDD-PRS与TBI后抑郁症之间的重叠性较弱。PRS可以改善风险预测,并为干预试验提供富集。
本研究得到了欧盟FP7资助、汉内洛尔·科尔基金会、英特格拉生命科学公司、神经创伤科学公司、美国国立卫生研究院、美国国防部、国家橄榄球联盟咨询委员会、美国能源部和One Mind的资助。