Martínez-Montoro José Ignacio, Cornejo-Pareja Isabel, Díaz-López Andrés, Sureda Antoni, Toledo Estefania, Abete Itziar, Babio Nancy, Tur Josep A, Martinez-Gonzalez Miguel A, Martínez J Alfredo, Fitó Montse, Salas-Salvadó Jordi, Tinahones Francisco J
Department of Endocrinology and Nutrition, Virgen de la Victoria University Hospital, Málaga, Spain.
Instituto de Investigación Biomédica de Málaga (IBIMA)-Plataforma BIONAND, Málaga, Spain.
J Intern Med. 2025 Feb;297(2):141-155. doi: 10.1111/joim.20038. Epub 2024 Dec 26.
Large-scale trials evaluating a multicomponent lifestyle intervention aimed at weight loss on kidney function are lacking.
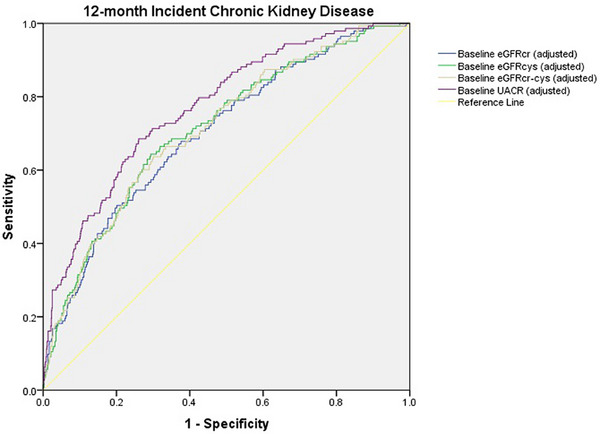
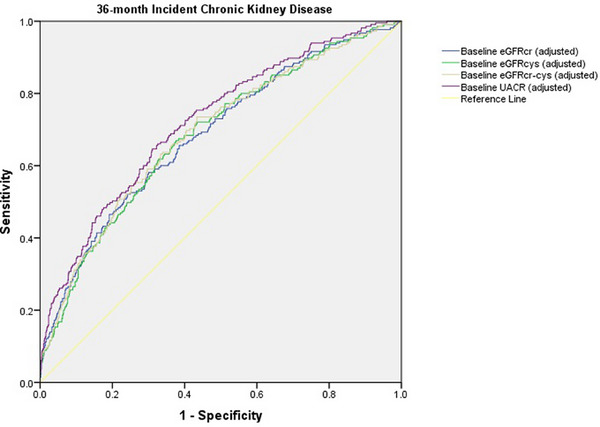
This was a post hoc analysis of the "PREvención con DIeta MEDiterránea-Plus" (PREDIMED-Plus) randomized controlled trial, including patients with overweight/obesity and metabolic syndrome, measured cystatin C and creatinine. Participants were randomly assigned (1:1) to an intensive weight loss lifestyle intervention (intervention group [IG]) consisting of an energy-restricted Mediterranean diet (MedDiet), physical activity promotion and behavioral support, or a control group (CG) receiving ad libitum MedDiet recommendations. The primary outcome was between-group differences in cystatin C-based kidney function (cystatin C-based estimated glomerular filtration rate-eGFRcys-and combined cystatin C-creatinine-based eGFR-eGFRcr-cys) change from baseline to 12 and 36 months. Secondary outcomes included between-group differences in creatinine-based eGFR (eGFRcr) and urinary albumin-to-creatinine ratio (UACR) change and the predictive capacity of these formulas at baseline for new-onset chronic kidney disease (CKD).
A total of 1909 participants (65 ± 5 years, 54% men) were included. Twelve-month decline in eGFRcys, eGFRcr-cys, and eGFRcr was greater in the CG compared to the IG, with between-group differences of -1.77 mL/min/1.73 m [95% confidence interval -2.92 to -0.63], -1.37 [-2.22 to -0.53], and -0.91 [-1.74 to -0.71], respectively. At 36 months, the decline in eGFRcr-cys and eGFRcr was greater in the CG. No between-group differences in UACR were found. Significant adjusted areas under the curve for baseline eGFRcys and eGFRcr-cys were observed for incident CKD at 36 months, which were similar to those for eGFRcr and UACR.
In older adults with overweight/obesity and metabolic syndrome, the PREDIMED-Plus intervention may be an optimal approach to preserve kidney function.
缺乏评估旨在减重的多成分生活方式干预对肾功能影响的大规模试验。
这是对“地中海饮食预防加量”(PREDIMED-Plus)随机对照试验的事后分析,纳入超重/肥胖和代谢综合征患者,检测胱抑素C和肌酐。参与者被随机分配(1:1)至强化减重生活方式干预组(干预组[IG]),该组采用能量限制的地中海饮食(MedDiet)、促进身体活动及行为支持,或对照组(CG),后者接受随意的MedDiet建议。主要结局是从基线至12个月和36个月时,基于胱抑素C的肾功能(基于胱抑素C的估计肾小球滤过率 - eGFRcys - 以及基于胱抑素C和肌酐的联合eGFR - eGFRcr - cys)在组间的差异。次要结局包括基于肌酐的eGFR(eGFRcr)和尿白蛋白与肌酐比值(UACR)在组间的变化,以及这些公式在基线时对新发慢性肾脏病(CKD)的预测能力。
共纳入1909名参与者(65±5岁,54%为男性)。与IG相比,CG中eGFRcys、eGFRcr - cys和eGFRcr在12个月时的下降更大,组间差异分别为 -1.77 mL/min/1.73m [95%置信区间 -2.92至 -0.63]、-1.37 [-2.22至 -0.53]和 -0.91 [-1.74至 -0.71]。在36个月时,CG中eGFRcr - cys和eGFRcr的下降更大。未发现UACR在组间存在差异。在36个月时,观察到基线eGFRcys和eGFRcr - cys对于新发CKD的曲线下显著调整面积,与eGFRcr和UACR的相似。
在患有超重/肥胖和代谢综合征的老年人中,PREDIMED-Plus干预可能是保护肾功能的最佳方法。