Khaled Maram, Baranov Adriana, Diaz Alvaro, Patel Mansi, Clements Sarah, Farsinejad Parsa, Khatana Kabir, Gnanapragasam Ashmitha, Selvanayagam Sathurthika, Muhsen Zeineb, Chan Jocelyn, Hunjan Sanjum, Kazi Ayman, Sharma Sapna, Luketic Lea, Ewusie Joycelyne Efua, Cordovani Daniel, Shanthanna Harsha
Department of Anesthesia, McMaster University, Hamilton, Ontario, Canada.
Perioperative and Surgery Research Program, Population Health Research Institute, Hamilton, Ontario, Canada.
PLoS One. 2024 Dec 26;19(12):e0314010. doi: 10.1371/journal.pone.0314010. eCollection 2024.
Caesarean section (CS) is the most common inpatient surgical procedure performed in Canada. CS is known to cause moderate-to-severe pain, which is suggested to be associated with postpartum depression and persistent pain. Existing limitations in multimodal analgesia and conscious attempts to avoid opioids highlight the need for non-pharmacological strategies. Photobiomodulation therapy (PBMT) uses light-emitting diode (LED) and laser and has suggested potential for improving pain control and wound healing. This study aims to evaluate the effectiveness of PBMT as part of existing multimodal analgesia after elective CSs.
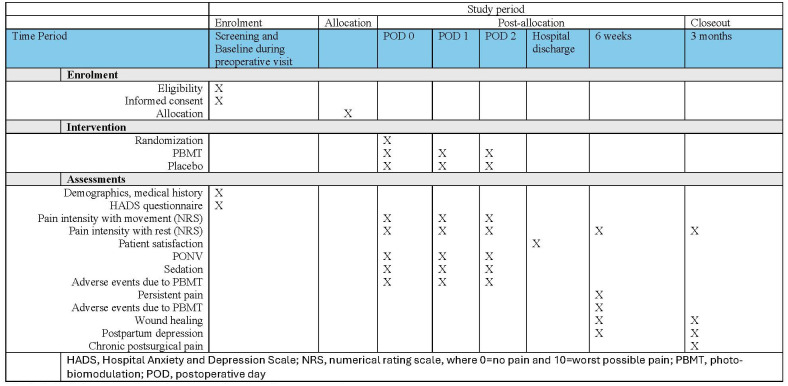
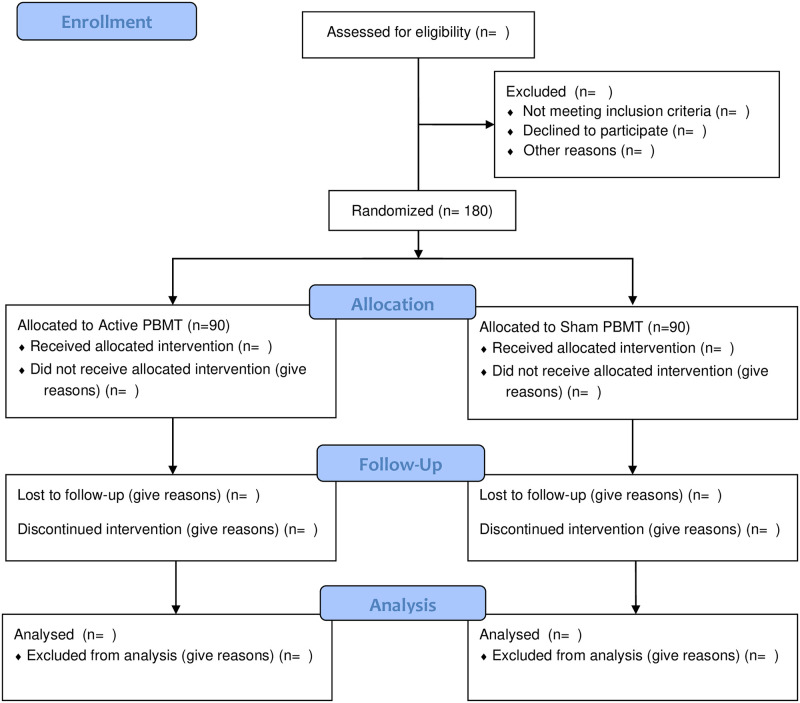
This placebo-controlled, two-arm, multi-centre, parallel-design randomized controlled trial includes women aged ≥16 years with planned CS under spinal anesthesia (Clinical Trials Registration: NCT05738239). Patients will be randomized post-CS to intervention (n = 90) or placebo (n = 90). Study interventions will be carried out using equipment supported by Meditech International Incorporated (approved by Health Canada for pain relief). Patients will receive a maximum of 5 post-surgical treatment sessions of active PBMT (intervention: LED therapy: DUO 240 [red at 660nm and near-infrared at 840nm] applied parallel to the abdominal incision scar, followed by BIOFLEX LDR-100 laser probe (660nm red light) and the LD1-200 laser probe (825nm near-infrared light), applied at the incision wound edges) or non-effective doses of LED array and laser therapy (placebo), 4-6 hrs post-CS, and at 8am and 7pm of postoperative days 1 and 2. Patients, research assistants involved in patient recruitment and follow-up, health care providers, and data analysts will be blinded. All patients will have access to routine multimodal analgesia. Patients will be followed up in hospital on the evening of surgery and on postoperative days 1 and 2 (morning, noon, and evening); at 6 weeks; and at 3 months by telephone. Primary outcome is pain intensity with movement (elicited by asking the patient to move from supine to sitting position) using 0-10 Numerical Rating Scale (0 = no pain, 10 = worst possible pain).
The results of this study may result in improved pain control, maternal satisfaction and wound healing; decrease the use of perioperative opioids; potentially decrease the incidence of postpartum depression and persistent pain; and overall lead to better postoperative outcomes thereby decreasing healthcare costs.
剖宫产术(CS)是加拿大最常见的住院手术。已知剖宫产会导致中度至重度疼痛,这被认为与产后抑郁和持续性疼痛有关。多模式镇痛的现有局限性以及避免使用阿片类药物的有意识尝试凸显了非药物策略的必要性。光生物调节疗法(PBMT)使用发光二极管(LED)和激光,已显示出改善疼痛控制和伤口愈合的潜力。本研究旨在评估PBMT作为择期剖宫产术后现有多模式镇痛一部分的有效性。
这项安慰剂对照、双臂、多中心、平行设计的随机对照试验纳入年龄≥16岁、计划在脊髓麻醉下进行剖宫产的女性(临床试验注册号:NCT05738239)。患者将在剖宫产术后随机分为干预组(n = 90)或安慰剂组(n = 90)。研究干预将使用Meditech International Incorporated公司支持的设备进行(经加拿大卫生部批准用于缓解疼痛)。患者将在术后接受最多5次主动PBMT治疗(干预:LED疗法:DUO 240[660nm红光和840nm近红外光]平行于腹部切口疤痕应用,随后使用BIOFLEX LDR - 100激光探头(660nm红光)和LD1 - 200激光探头(825nm近红外光),应用于切口伤口边缘)或无效剂量的LED阵列和激光疗法(安慰剂),在剖宫产术后4 - 6小时以及术后第1天和第2天的上午8点和晚上7点进行。患者、参与患者招募和随访的研究助理、医疗保健提供者以及数据分析人员将被设盲。所有患者都可接受常规多模式镇痛。患者将在手术当晚、术后第1天和第2天(上午、中午和晚上)、6周时以及3个月时通过电话进行随访。主要结局是使用0 - 10数字评分量表(0 = 无疼痛,10 = 可能的最严重疼痛)评估患者从仰卧位变为坐位时的运动疼痛强度。
本研究结果可能会改善疼痛控制、产妇满意度和伤口愈合;减少围手术期阿片类药物的使用;潜在降低产后抑郁和持续性疼痛的发生率;并总体上带来更好的术后结局,从而降低医疗成本。