Mehmedbegovic Zlatko, Vukcevic Vladan, Stojkovic Sinisa, Beleslin Branko, Orlic Dejan, Tomasevic Miloje, Dikic Miodrag, Tesic Milorad, Milasinovic Dejan, Aleksandric Srdjan, Dedovic Vladimir, Zivkovic Milorad, Juricic Stefan, Jelic Dario, Mladenovic Djordje, Stankovic Goran
Department of Cardiology, University Clinical Center of Serbia, 11000 Belgrade, Serbia.
Faculty of Medicine, University of Belgrade, 11000 Belgrade, Serbia.
Rev Cardiovasc Med. 2024 Dec 19;25(12):445. doi: 10.31083/j.rcm2512445. eCollection 2024 Dec.
Elective unprotected left main (ULM) percutaneous coronary intervention (PCI) has long-term mortality rates comparable to surgical revascularization, thanks to advances in drug-eluting stent (DES) design, improved PCI techniques, and frequent use of intravascular imaging. However, urgent PCI of ULM culprit lesions remains associated with high in-hospital mortality and unfavourable long-term outcomes, including DES restenosis and stent thrombosis (ST). This analysis aimed to examine the long-term outcomes and healing of DES implanted in ULM during primary PCI using high-resolution optical coherence tomography (OCT) imaging.
A total of 15 consecutive patients undergoing long-term OCT follow-up of ULM primary PCI from a high-volume center were included in this analysis. During the index primary PCI all subjects underwent angio-guided DES implantation, and follow-up was uneventful in all but one subject who had a non-target PCI lesion. The primary endpoint was the percentage of covered, uncovered, and malappossed stent struts at long-term follow-up. Secondary endpoints included quantitative and qualitative OCT measurements. For the left main bifurcation, a separate analysis was performed for three different segments: left main (LM), polygon of confluence (POC) and distal main branch (dMB), in all cases.
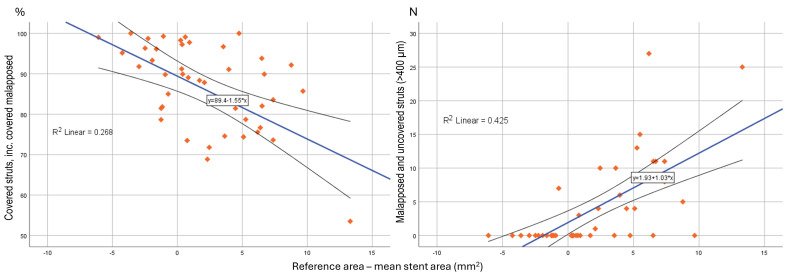
The average follow-up interval until OCT was 1580 ± 1260 days. Despite aorto-ostial stent protrusions in 40% of patients, optimal image quality was achieved in 93.3% of cases. There were higher rates of malapposed (11.4 ± 16.6 vs. 13.1 ± 8.3 vs. 0.3 ± 0.5%; < 0.001) and lower rates of covered struts (81.7 ± 16.8 vs. 83.7 ± 9.2 vs. 92.4 ± 6.8%; = 0.041) observed for the LM and POC segment compared to the dMB. Significantly malapposed stent struts (>400 μm) were less likely to be covered at follow-up, than struts with a measured strut to vessel wall distance of <400 μm (15.4 ± 21.6 vs. 24.8 ± 23.9%; = 0.011). Neoatherosclerosis was observed in 5 (33.3%) and restenotic neointimal hyperplasia (NIH) in 2 (13.3%) patients, requiring PCI in 33.3% of patients.
Long-term OCT examination of DES implanted during primary PCI for culprit ULM lesions demonstrated high rates of incomplete strut coverage, late malapposition, and high subclinical DES failure rates. These negative OCT results highlight the need for image optimization strategies during primary PCI to improve DES-related long-term outcomes.
由于药物洗脱支架(DES)设计的进步、PCI技术的改进以及血管内成像的频繁使用,择期无保护左主干(ULM)经皮冠状动脉介入治疗(PCI)的长期死亡率与外科血运重建相当。然而,ULM罪犯病变的急诊PCI仍然与高院内死亡率和不良的长期预后相关,包括DES再狭窄和支架血栓形成(ST)。本分析旨在使用高分辨率光学相干断层扫描(OCT)成像检查在原发性PCI期间植入ULM的DES的长期预后和愈合情况。
本分析纳入了来自一个高容量中心的15例连续接受ULM原发性PCI长期OCT随访的患者。在首次原发性PCI期间,所有受试者均接受了血管造影引导下的DES植入,除1例有非靶PCI病变的受试者外,所有受试者的随访均顺利。主要终点是长期随访时覆盖、未覆盖和贴壁不良的支架支柱百分比。次要终点包括定量和定性OCT测量。对于左主干分叉,在所有病例中对三个不同节段:左主干(LM)、汇合区(POC)和远端主支(dMB)进行了单独分析。
直到进行OCT的平均随访间隔为1580±1260天。尽管40%的患者存在主动脉开口处支架突出,但93.3%的病例获得了最佳图像质量。与dMB相比,LM和POC节段观察到贴壁不良率更高(11.4±16.6 vs.13.1±8.3 vs.0.3±0.5%;P<0.001),覆盖支柱率更低(81.7±16.8 vs.83.7±9.2 vs.92.4±6.8%;P = 0.041)。与测量的支柱到血管壁距离<400μm的支柱相比,显著贴壁不良的支架支柱(>400μm)在随访时被覆盖的可能性更小(15.4±21.6 vs.24.8±23.9%;P = 0.011)。5例(33.3%)患者观察到新生动脉粥样硬化,2例(13.3%)患者观察到再狭窄性新生内膜增生(NIH),33.3%的患者需要进行PCI。
对罪犯ULM病变进行原发性PCI期间植入的DES进行长期OCT检查显示,支架支柱覆盖不完全、晚期贴壁不良和亚临床DES失败率高。这些负面的OCT结果突出了在原发性PCI期间需要图像优化策略以改善DES相关的长期预后。