Thompson Jacqueline, Watson Samuel I, Middleton Lee, Hemming Karla
Department of Applied Health Sciences, College of Medicine and Health, University of Birmingham, Edgbaston, West Midlands, B15 2TT, UK.
Trials. 2025 Jan 2;26(1):1. doi: 10.1186/s13063-024-08690-w.
Guidelines for randomised controlled trials (RCTs) recommend reporting relative and absolute measures of effect for binary outcomes while adjusting for covariates. There are a number of different ways covariate-adjusted relative risks and risk differences can be estimated.
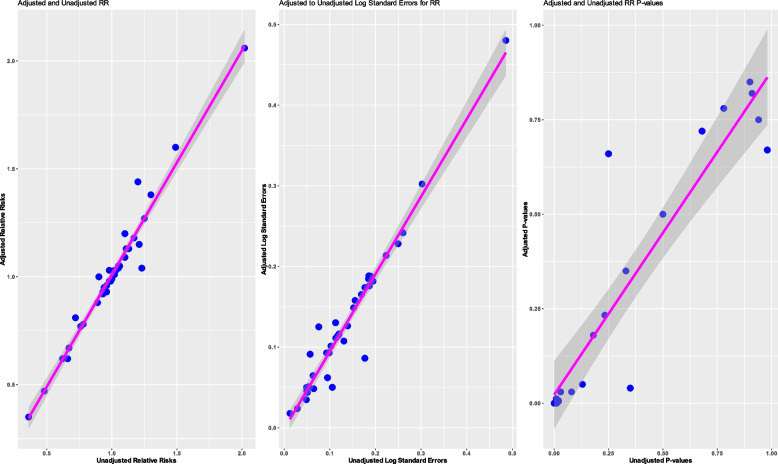
Our goal was to identify methods used to estimate covariate-adjusted relative risk and risk differences in RCTs published in high-impact journals with binary outcomes. Other secondary objectives included the identification of how covariates are chosen for adjustment and whether covariate adjustment results in an increase in statistical precision in practice.
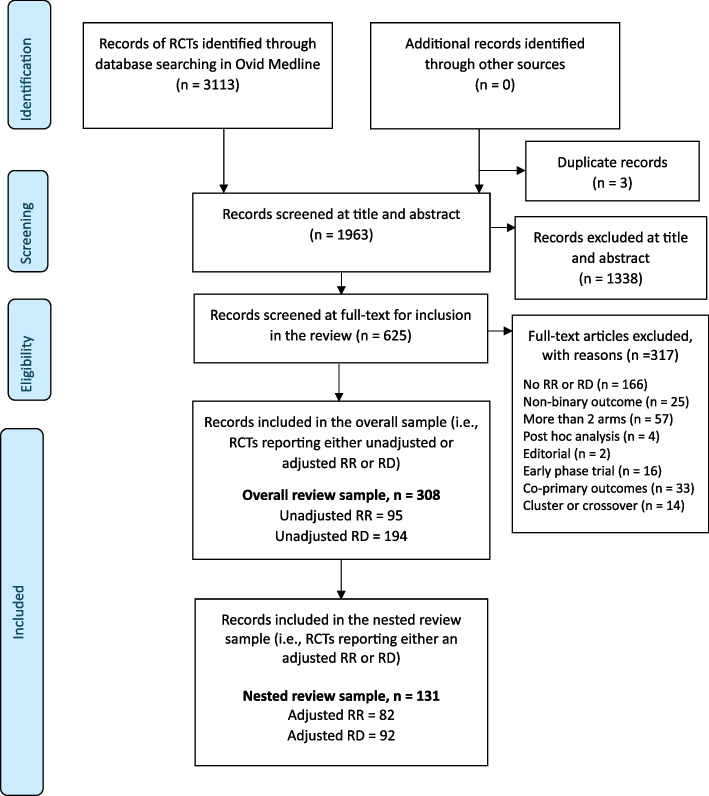
We included two-arm parallel RCTs published in JAMA, NEJM, Lancet, or the BMJ between January 1, 2018, and March 11, 2023, reporting relative risks or risk differences as a summary measure for a binary primary outcome. The search was conducted in Ovid-MEDLINE.
Of the 308 RCTs identified, around half (49%; 95% CI: 43-54%) reported a covariate-adjusted relative risk or risk difference. Of these, 82 reported an adjusted relative risk. When the reporting was clear (n = 65, 79%), the log-binomial model (used in 65% of studies; 95% CI: 52-76%) and modified Poisson (29%; 95% CI: 19-42%) were most commonly used. Of the 92 studies that reported an adjusted risk difference, when the reporting was clear (n = 56, 61%), the binomial model (used in 48% of studies; 95% CI: 35-62%) and marginal standardisation (21%; 95% CI: 12-35%) were the common approaches used.
Approximately half of the RCTs report either a covariate-adjusted relative risk or risk difference. Many RCTs lack adequate details on the methods used to estimate covariate-adjusted effects. Of those that do report the approaches used, the binomial model, modified Poisson and to a lesser extent marginal standardisation are the approaches used.
随机对照试验(RCT)指南建议在对协变量进行调整时,报告二元结局的效应的相对和绝对测量值。有多种不同的方法可用于估计经协变量调整的相对风险和风险差异。
我们的目标是确定在具有二元结局的高影响力期刊上发表的RCT中,用于估计经协变量调整的相对风险和风险差异的方法。其他次要目标包括确定如何选择协变量进行调整,以及在实际中协变量调整是否会提高统计精度。
我们纳入了2018年1月1日至2023年3月11日期间在《美国医学会杂志》(JAMA)、《新英格兰医学杂志》(NEJM)、《柳叶刀》(Lancet)或《英国医学杂志》(BMJ)上发表的双臂平行RCT,这些研究报告了相对风险或风险差异作为二元主要结局的汇总测量值。检索在Ovid-MEDLINE中进行。
在识别出的308项RCT中,约一半(49%;95%置信区间:43-54%)报告了经协变量调整的相对风险或风险差异。其中,82项报告了调整后的相对风险。当报告清晰时(n = 65,7�%),对数二项模型(65%的研究使用;95%置信区间:52-76%)和修正泊松模型(29%;95%置信区间:19-42%)是最常用的。在报告调整后风险差异的92项研究中,当报告清晰时(n = 56,61%),二项模型(48%的研究使用;95%置信区间:35-62%)和边际标准化(21%;95%置信区间:12-35%)是常用的方法。
约一半的RCT报告了经协变量调整的相对风险或风险差异。许多RCT缺乏关于用于估计经协变量调整效应的方法的充分细节。在那些确实报告了所使用方法的研究中,二项模型、修正泊松模型以及在较小程度上的边际标准化是所使用的方法。