Sharif Ben, Nana Melanie, Kearns Rachel, Lo Queenie, Metodiev Yavor
Department of Anaesthesia, University Hospital of Wales, Cardiff, UK.
Department of Obstetric Medicine, St Thomas' Hospital, London, UK.
Anaesthesia. 2025 Feb;80 Suppl 2(Suppl 2):115-124. doi: 10.1111/anae.16489. Epub 2025 Jan 8.
Cancer complicates approximately 1 in 2000 pregnancies, with increasing incidence due to factors such as increased maternal age, obesity and advancements in antenatal testing. Anaesthetists play a crucial role in managing pregnant patients with cancer, both during delivery and in providing anaesthesia for oncological treatments. This review explores the challenges in anaesthetic management and specific considerations for common cancers encountered in pregnant patients.
An electronic literature search was carried out using PubMed and Google Scholar to identify peer-reviewed articles published in English from 1 January 1990 to 30 July 2024.
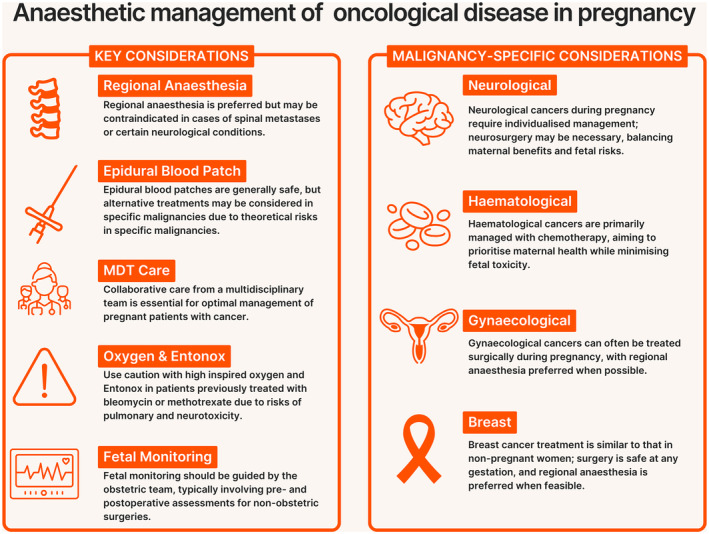
Two main areas were identified: anaesthetic management related to pregnancy and the peripartum period in patients with cancer; and oncological management during pregnancy. Current data suggest that pregnancy does not worsen cancer prognosis, but diagnosis and treatment are complicated by the overlap of cancer symptoms with physiological changes of pregnancy and concerns about the safety of diagnostic procedures and treatments. Ultrasound and magnetic resonance imaging are preferred imaging modalities, while careful use of ionising radiation is advised. Treatment during pregnancy, including surgery, chemotherapy and radiotherapy is possible, with specific timing and modality considerations to ensure maternal and fetal safety. Anaemia, poor nutrition and preterm birth are significant concerns in managing pregnant patients with cancer. For operative births, neuraxial techniques are preferred, though general anaesthesia may be required in complex cases. Comprehensive multidisciplinary support, including psychosocial care, is essential for optimal outcomes. Oncological surgery during pregnancy should preferably be scheduled for the second trimester, with consideration for fetal monitoring and steroids. Regional anaesthesia should be utilised if possible and uteroplacental perfusion maintained. Increased risks of thromboembolism should be addressed postoperatively, along with psychological support.
Effective and safe anaesthetic management of cancer in pregnancy requires a multidisciplinary approach to balance maternal and fetal safety, with a focus on careful planning and individualised care.
癌症在每2000例妊娠中约有1例并发,由于产妇年龄增加、肥胖和产前检查技术进步等因素,其发病率呈上升趋势。麻醉医生在管理患有癌症的孕妇方面发挥着关键作用,无论是在分娩期间还是为肿瘤治疗提供麻醉时。本综述探讨了麻醉管理中的挑战以及妊娠患者常见癌症的特殊注意事项。
使用PubMed和谷歌学术进行电子文献检索,以识别1990年1月1日至2024年7月30日期间以英文发表的同行评审文章。
确定了两个主要领域:癌症患者妊娠及围产期的麻醉管理;妊娠期间的肿瘤管理。目前的数据表明,妊娠不会恶化癌症预后,但癌症症状与妊娠生理变化的重叠以及对诊断程序和治疗安全性的担忧使诊断和治疗变得复杂。超声和磁共振成像为首选的成像方式,同时建议谨慎使用电离辐射。妊娠期间可以进行包括手术、化疗和放疗在内的治疗,但需要考虑特定的时机和方式以确保母婴安全。贫血、营养不良和早产是管理患有癌症的孕妇时的重大问题。对于手术分娩,首选神经轴技术,尽管在复杂病例中可能需要全身麻醉。全面的多学科支持,包括心理社会护理,对于实现最佳结果至关重要。妊娠期间的肿瘤手术最好安排在孕中期,同时考虑胎儿监测和使用类固醇。如有可能应使用区域麻醉并维持子宫胎盘灌注。术后应处理血栓栓塞风险增加的问题,并提供心理支持。
妊娠期癌症的有效和安全麻醉管理需要多学科方法来平衡母婴安全,重点是精心规划和个体化护理。