Lal Hira, Ruidas Surojit, Prasad Raghunandan, Singh Anuradha, Prasad Narayan, Kaul Anupma, Bhadauria Dharmendra S, Kushwaha Ravi S, Patel Manas R, Jain Manoj, Yadav Priyank
Department of Radiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226014, Uttar Pradesh, India.
Department of Nephrology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226014, Uttar Pradesh, India.
World J Radiol. 2024 Dec 28;16(12):782-793. doi: 10.4329/wjr.v16.i12.782.
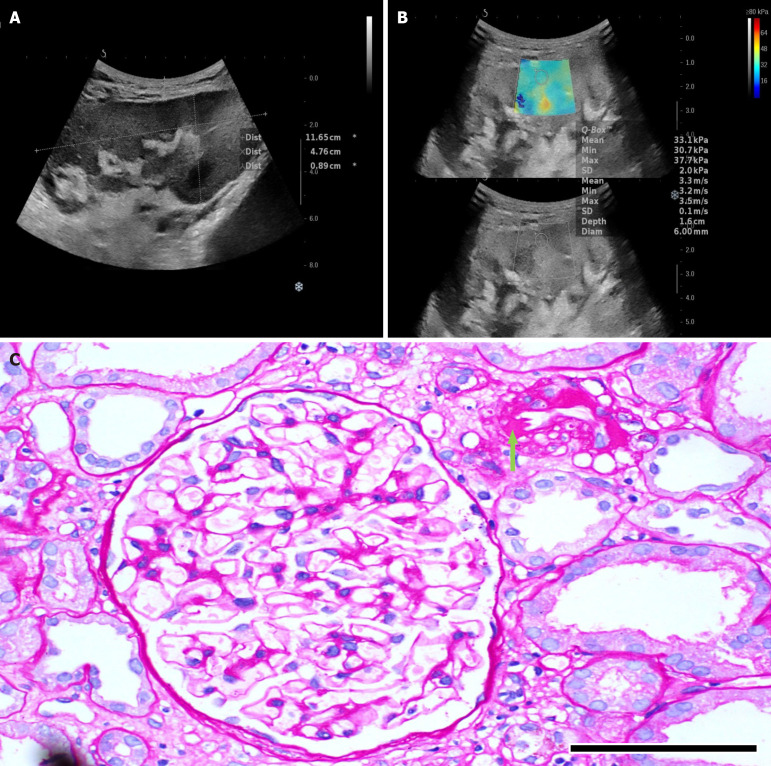
The study focuses on the use of multi-parametric ultrasound [gray scale, color Doppler and shear wave elastography (SWE)] to differentiate stable renal allografts from acute graft dysfunction and to assess time-dependent changes in parenchymal stiffness, thereby assessing its use as an efficient monitoring tool for ongoing graft dysfunction. To date, biopsy is the gold standard for evaluation of acute graft dysfunction. However, because it is invasive, it carries certain risks and cannot be used for follow-up monitoring. SWE is a non-invasive imaging modality that identifies higher parenchymal stiffness values in cases of acute graft dysfunction compared to stable grafts.
To assess renal allograft parenchymal stiffness by SWE and to correlate its findings with functional status of the graft kidney.
This prospective observational study included 71 renal allograft recipients. Multi-parametric ultrasound was performed on all patients, and biopsies were performed in cases of acute graft dysfunction. The study was performed for a period of 2 years at Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, a tertiary care center in north India. Independent samples -test was used to compare the means between two independent groups. Paired-samples -test was used to test the change in mean value between baseline and follow-up observations.
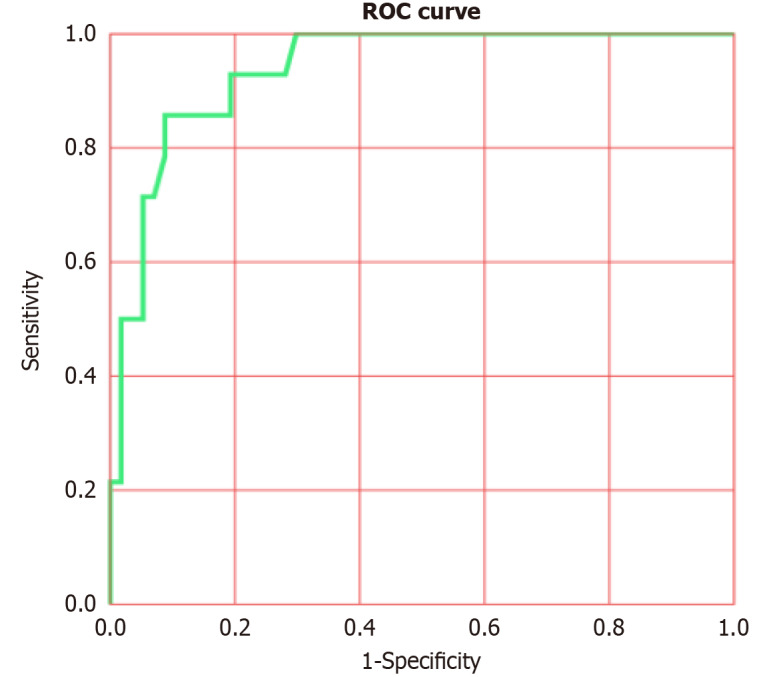
Thirty-one patients had experienced acute graft dysfunction at least once, followed by recovery, but none of them had a history of chronic renal allograft injury. Mean baseline parenchymal stiffness in stable grafts and acute graft dysfunction were 30.21 + 2.03 kPa (3.17 + 0.11 m/s) and 31.07 + 2.88 kPa (3.22 + 0.15 m/s), respectively; however, these differences were not statistically significant ( = 0.305 and 0.252, respectively). There was a gradual decrease in SWE values during the first 3 postoperative months, followed by an increase in SWE values up to one-year post-transplantation. Patients with biopsy-confirmed graft dysfunction showed higher SWE values compared to those with a negative biopsy. However, receiver operating characteristic analysis failed to show statistically significant cut-off values to differentiate between the stable graft and acute graft dysfunction.
Acute graft dysfunction displays higher parenchymal stiffness values compared to stable grafts. Therefore, SWE may be useful in monitoring the functional status of allografts to predict any ongoing dysfunction.
本研究聚焦于运用多参数超声[灰阶、彩色多普勒及剪切波弹性成像(SWE)]来区分稳定的肾移植与急性移植肾功能障碍,并评估实质硬度随时间的变化,从而评估其作为持续移植肾功能障碍有效监测工具的用途。迄今为止,活检是评估急性移植肾功能障碍的金标准。然而,由于其具有侵入性,存在一定风险且不能用于随访监测。SWE是一种非侵入性成像方式,与稳定移植相比,其在急性移植肾功能障碍病例中可识别出更高的实质硬度值。
通过SWE评估肾移植实质硬度,并将其结果与移植肾的功能状态相关联。
这项前瞻性观察性研究纳入了71名肾移植受者。对所有患者进行了多参数超声检查,对于急性移植肾功能障碍患者进行了活检。该研究在印度北部三级医疗中心勒克瑙的桑贾伊·甘地医学科学研究生学院进行了2年。采用独立样本t检验比较两个独立组之间的均值。采用配对样本t检验来检验基线与随访观察之间均值的变化。
31名患者至少经历过一次急性移植肾功能障碍,随后恢复,但他们均无慢性肾移植损伤史。稳定移植组和急性移植肾功能障碍组的平均基线实质硬度分别为30.21 + 2.03 kPa(3.17 + 0.11 m/s)和31.07 + 2.88 kPa(3.22 + 0.15 m/s);然而,这些差异无统计学意义(分别为 = 0.305和0.252)。术后前3个月SWE值逐渐下降,随后直至移植后1年SWE值升高。活检证实有移植肾功能障碍的患者与活检阴性的患者相比,SWE值更高。然而,受试者工作特征分析未能显示出区分稳定移植与急性移植肾功能障碍的具有统计学意义的临界值。
与稳定移植相比,急性移植肾功能障碍表现出更高的实质硬度值。因此,SWE可能有助于监测移植肾的功能状态以预测任何持续的功能障碍。