Rouby Jean-Jacques, Xia Jing, Dhanani Jayesh, Bassi Gianluigi Li, Monsel Antoine, Torres Antoni
Department of Anaesthesiology and Critical Care, Sorbonne University, GRC 29, Assistance Publique Hôpitaux de Paris (AP-HP), DMU DREAM, Multidisciplinary Intensive Care Unit, Pitié-Salpêtrière Hospital, Paris, France.
Emergency Department, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, China.
J Intensive Med. 2024 Oct 16;5(1):12-22. doi: 10.1016/j.jointm.2024.07.006. eCollection 2025 Jan.
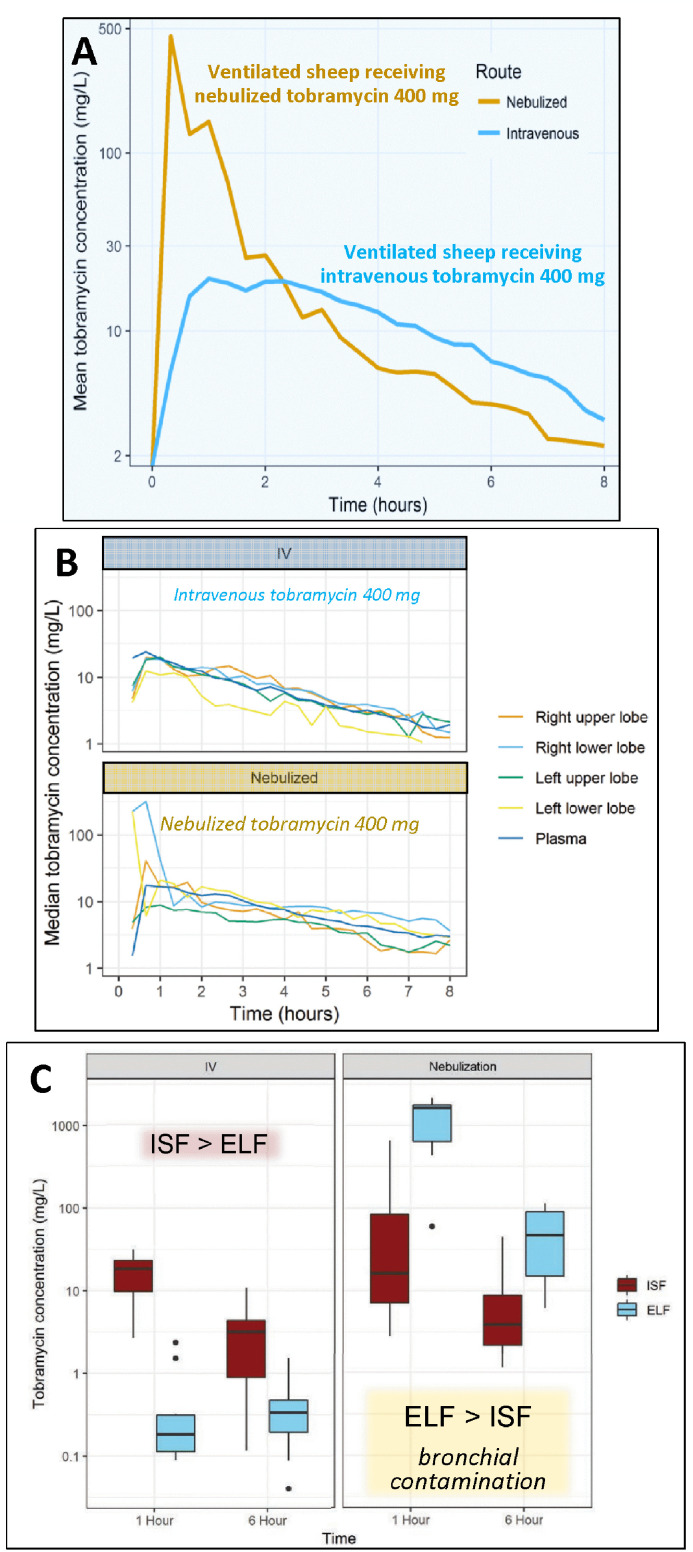
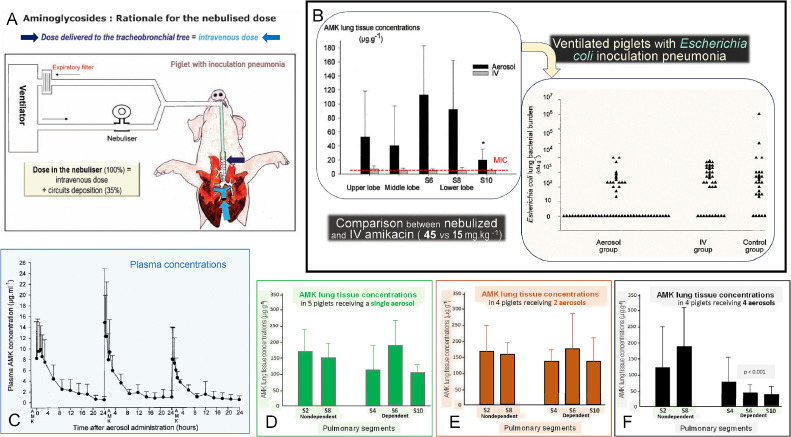
Aminoglycosides are concentration-dependent antibiotics exerting a bactericidal effect when concentrations at the site of infection are equal to or greater than 5 times the minimum inhibitory concentrations (MIC). When administered intravenously, they exhibit poor lung penetration and high systemic renal and ototoxicity, imposing to restrict their administration to 5 days. Experimental studies conducted in anesthetized and mechanically ventilated sheep and pigs provide evidence that high doses of nebulized aminoglycosides induce a rapid and potent bacterial killing in the infected lung parenchyma. They also confirm that the alveolar-capillary membrane, either normal or injured by the infectious process, restricts the penetration of intravenous aminoglycosides in the infected lung parenchyma, precluding a bactericidal effect at the site of infection. However, injury of the alveolar-capillary membrane promotes the systemic diffusion of nebulized aminoglycosides. Based on experimental data obtained in animals with inoculation pneumonia, it challenges the classical belief that nebulization protects against systemic toxicity. Loss of lung aeration decreases the lung penetration of nebulized aminoglycosides. Nevertheless, lung tissue concentrations measured in non-aerated lung regions with severe and extended pneumonia are most often greater than 5 times the MICs, resulting in a bactericidal effect followed by a progressive pulmonary reaeration. It is likely that the penetration into the consolidated lung, results from the bronchial diffusion of nebulized aminoglycosides toward adjacent non-aerated infected alveolar spaces and their penetration into mechanical ventilation-induced intraparenchymal pseudocysts and distended bronchioles. In animals receiving nebulized aminoglycosides, epithelial lining fluid concentrations grossly overestimate lung interstitial fluid concentrations because of the bronchial contamination of the distal tip of the bronchoscope during the bronchoalveolar procedures. Lung microdialysis is the only technique able to accurately assess lung pharmacokinetics in animals with inoculation pneumonia treated by nebulized aminoglycosides. In 2024, the European Investigators Network for Nebulized Antibiotics in Ventilator-associated Pneumonia (ENAVAP) called for the creation of an international research network for Lung Microdialysis applied to Nebulized Antibiotics (LUMINA) to promote multicentered, experimental, randomized, and controlled studies addressing lung pharmacokinetics of intravenous vs. nebulized antibiotics, using different dosing and ventilator settings.
氨基糖苷类是浓度依赖性抗生素,当感染部位的浓度等于或大于最低抑菌浓度(MIC)的5倍时发挥杀菌作用。静脉给药时,它们在肺部的渗透较差,且具有较高的全身肾毒性和耳毒性,因此给药期限被限制为5天。在麻醉并机械通气的绵羊和猪身上进行的实验研究表明,高剂量雾化氨基糖苷类可在受感染的肺实质中迅速产生强效杀菌作用。这些研究还证实,无论是正常的还是因感染过程受损的肺泡 - 毛细血管膜,都会限制静脉注射氨基糖苷类药物进入受感染的肺实质,从而无法在感染部位发挥杀菌作用。然而,肺泡 - 毛细血管膜的损伤会促进雾化氨基糖苷类药物的全身扩散。基于接种性肺炎动物的实验数据,这对雾化可预防全身毒性的传统观念提出了挑战。肺通气减少会降低雾化氨基糖苷类药物在肺部的渗透。尽管如此,在患有严重且广泛肺炎的无通气肺区域测得的肺组织浓度通常大于MIC的5倍,从而产生杀菌作用,随后肺部逐渐恢复通气。雾化氨基糖苷类药物进入实变肺的原因可能是,其通过支气管扩散到相邻的无通气感染肺泡空间,并进入机械通气引起的肺实质内假囊肿和扩张的细支气管。在接受雾化氨基糖苷类药物的动物中,由于支气管肺泡操作期间支气管镜远端受到支气管污染,上皮衬液浓度严重高估了肺间质液浓度。肺微透析是唯一能够准确评估雾化氨基糖苷类药物治疗接种性肺炎动物肺药代动力学的技术。2024年,欧洲呼吸机相关性肺炎雾化抗生素研究人员网络(ENAVAP)呼吁创建一个应用于雾化抗生素的肺微透析国际研究网络(LUMINA),以促进多中心、实验性、随机对照研究,探讨静脉注射与雾化抗生素在不同给药剂量和呼吸机设置下的肺药代动力学。