Guglielmetti Lorenzo, Khan Uzma, Velásquez Gustavo E, Gouillou Maelenn, Abubakirov Amanzhan, Baudin Elisabeth, Berikova Elmira, Berry Catherine, Bonnet Maryline, Cellamare Matteo, Chavan Vijay, Cox Vivian, Dakenova Zhanna, de Jong Bouke Catherine, Ferlazzo Gabriella, Karabayev Aydarkhan, Kirakosyan Ohanna, Kiria Nana, Kunda Mikanda, Lachenal Nathalie, Lecca Leonid, McIlleron Helen, Motta Ilaria, Toscano Sergio Mucching, Mushtaque Hebah, Nahid Payam, Oyewusi Lawrence, Panda Samiran, Patil Sandip, Phillips Patrick P J, Ruiz Jimena, Salahuddin Naseem, Garavito Epifanio Sanchez, Seung Kwonjune J, Ticona Eduardo, Trippa Lorenzo, Vasquez Dante E Vargas, Wasserman Sean, Rich Michael L, Varaine Francis, Mitnick Carole D
From Médecins Sans Frontières (L.G., F.V.), Sorbonne Université, INSERM Unité 1135, Centre d'Immunologie et des Maladies Infectieuses (L.G.), Assistance Publique-Hôpitaux de Paris, Groupe Hospitalier Universitaire Sorbonne Université, Hôpital Pitié-Salpêtrière, Centre National de Référence des Mycobactéries et de la Résistance des Mycobactéries aux Antituberculeux (L.G.), and Epicentre (M.G., E. Baudin), Paris, and Translational Research on HIV and Endemic and Emerging Infectious Diseases, Montpellier Université de Montpellier, Montpellier, Institut de Recherche pour le Développement, Montpellier, INSERM, Montpellier (M.B.) - all in France; Interactive Development and Research, Singapore (U.K.); McGill University, Epidemiology, Biostatistics, and Occupational Health, Montreal (U.K.); UCSF Center for Tuberculosis (G.E.V., P.N., P.P.J.P.) and the Division of HIV, Infectious Diseases, and Global Medicine (G.E.V.), University of California at San Francisco, San Francisco; the National Scientific Center of Phthisiopulmonology (A.A., E. Berikova) and the Center of Phthisiopulmonology of Almaty Health Department (A.K.), Almaty, and the City Center of Phthisiopulmonology, Astana (Z.D.) - all in Kazakhstan; Médecins Sans Frontières (C.B., I.M.), the Medical Research Council Clinical Trials Unit at University College London (I.M.), and St. George's University of London Institute for Infection and Immunity (S.W.) - all in London; MedStar Health Research Institute, Washington, DC (M.C.); Médecins Sans Frontières, Mumbai (V. Chavan), the Indian Council of Medical Research Headquarters-New Delhi, New Delhi (S. Panda), and the Indian Council of Medical Research-National AIDS Research Institute, Pune (S. Patil) - all in India; the Centre for Infectious Disease Epidemiology and Research (V. Cox) and the Department of Medicine (H. McIlleron), University of Cape Town, and the Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine (S.W.) - both in Cape Town, South Africa; the Institute of Tropical Medicine, Antwerp, Belgium (B. C. J.); Médecins Sans Frontières, Geneva (G.F., N.L.); Médecins Sans Frontières, Yerevan, Armenia (O.K.); the National Center for Tuberculosis and Lung Diseases, Tbilisi, Georgia (N.K.); Partners In Health (M.K.) and Jhpiego Lesotho (L.O.) - both in Maseru; Socios En Salud Sucursal Peru (L.L., S.M.-T., J.R., E.S.-G., D.E.V.-V.), Hospital Nacional Sergio E. Bernales, Centro de Investigacion en Enfermedades Neumologicas (E.S.-G.), Hospital Nacional Dos de Mayo (E.T.), Universidad Nacional Mayor de San Marcos (E.T.), and Hospital Nacional Hipólito Unanue (D.E.V.-V.) - all in Lima; Global Health and Social Medicine, Harvard Medical School (L.L., K.J.S., M.L.R., C.D.M.), Partners In Health (L.L., K.J.S., M.L.R., C.D.M.), the Division of Global Health Equity, Brigham and Women's Hospital (K.J.S., M.L.R., C.D.M.), the Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, (L.T.), and Harvard T.H. Chan School of Public Health (L.T.) - all in Boston; and the Indus Hospital and Health Network, Karachi, Pakistan (H. Mushtaque, N.S.).
N Engl J Med. 2025 Jan 30;392(5):468-482. doi: 10.1056/NEJMoa2400327.
For decades, poor treatment options and low-quality evidence plagued care for patients with rifampin-resistant tuberculosis. The advent of new drugs to treat tuberculosis and enhanced funding now permit randomized, controlled trials of shortened-duration, all-oral treatments for rifampin-resistant tuberculosis.
We conducted a phase 3, multinational, open-label, randomized, controlled noninferiority trial to compare standard therapy for treatment of fluoroquinolone-susceptible, rifampin-resistant tuberculosis with five 9-month oral regimens that included various combinations of bedaquiline (B), delamanid (D), linezolid (L), levofloxacin (Lfx) or moxifloxacin (M), clofazimine (C), and pyrazinamide (Z). Participants were randomly assigned (with the use of Bayesian response-adaptive randomization) to receive one of five combinations or standard therapy. The primary end point was a favorable outcome at week 73, defined by two negative sputum culture results or favorable bacteriologic, clinical, and radiologic evolution. The noninferiority margin was -12 percentage points.
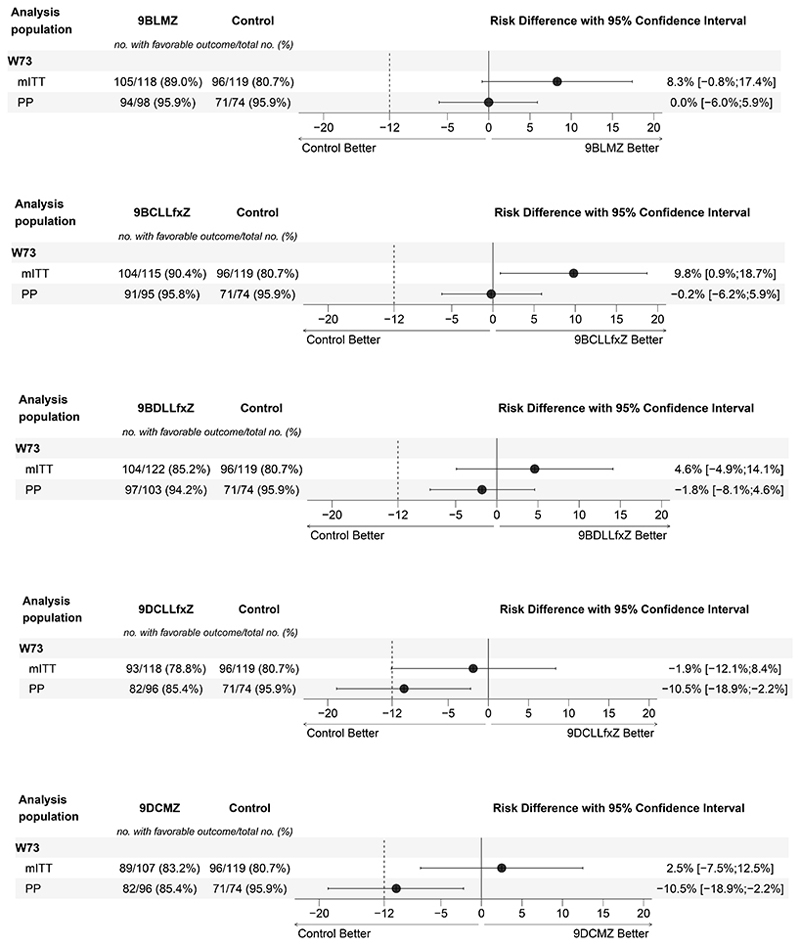
Among the 754 participants who underwent randomization, 699 were included in the modified intention-to-treat analysis, and 562 in the per-protocol analysis. In the modified intention-to-treat analysis, 80.7% of the patients in the standard-therapy group had favorable outcomes. The risk difference between standard therapy and each of the four new regimens that were found to be noninferior in the modified intention-to-treat population was as follows: BCLLfxZ, 9.8 percentage points (95% confidence interval [CI], 0.9 to 18.7); BLMZ, 8.3 percentage points (95% CI, -0.8 to 17.4); BDLLfxZ, 4.6 percentage points (95% CI, -4.9 to 14.1); and DCMZ, 2.5 percentage points (95% CI, -7.5 to 12.5). Differences were similar in the per-protocol population, with the exception of DCMZ, which was not noninferior in that population. The proportion of participants with grade 3 or higher adverse events was similar across the regimens. Grade 3 or higher hepatotoxic events occurred in 11.7% of participants overall and in 7.1% of those receiving standard therapy.
Consistent results across all the analyses support the noninferior efficacy of three all-oral shortened regimens for the treatment of rifampin-resistant tuberculosis. (Funded by Unitaid and others; endTB ClinicalTrials.gov number, NCT02754765.).
数十年来,治疗选择有限以及证据质量低下一直困扰着耐利福平结核病患者的治疗。新型抗结核药物的出现以及资金投入的增加,使得开展针对耐利福平结核病的短疗程全口服治疗的随机对照试验成为可能。
我们开展了一项3期、多国、开放标签、随机对照的非劣效性试验,以比较氟喹诺酮敏感、耐利福平结核病的标准治疗方案与五种9个月的口服方案,这五种方案包含不同组合的贝达喹啉(B)、地拉米啶(D)、利奈唑胺(L)、左氧氟沙星(Lfx)或莫西沙星(M)、氯法齐明(C)和吡嗪酰胺(Z)。参与者通过贝叶斯反应适应性随机化被随机分配,接受五种组合方案之一或标准治疗。主要终点为第73周时的良好结局,定义为两次痰培养结果阴性或细菌学、临床和影像学方面的良好进展。非劣效界值为-12个百分点。
在754名接受随机分组的参与者中,699名纳入了改良意向性分析,562名纳入了符合方案分析。在改良意向性分析中,标准治疗组80.7%的患者获得了良好结局。在改良意向性分析人群中被发现非劣效的标准治疗与四种新方案之间的风险差异如下:BCLLfxZ为9.8个百分点(95%置信区间[CI],0.9至18.7);BLMZ为8.3个百分点(95%CI,-0.8至17.4);BDLLfxZ为4.6个百分点(95%CI,-4.9至14.1);DCMZ为2.5个百分点(95%CI,-7.5至12.5)。在符合方案人群中的差异相似,但DCMZ在该人群中并非非劣效。各方案中3级或更高等级不良事件的参与者比例相似。总体上,11.7%的参与者发生了3级或更高等级的肝毒性事件,接受标准治疗的参与者中这一比例为7.1%。
所有分析结果一致,支持三种全口服短疗程方案治疗耐利福平结核病的非劣效疗效。(由国际药品采购机制等资助;endTB临床试验注册号,NCT02754765。)