MRC Clinical Trials Unit at UCL, London, UK.
University of Cape Town Lung Institute, Cape Town, South Africa; Division of Pulmonology, Department of Medicine, University of Cape Town, Cape Town, South Africa.
Lancet Respir Med. 2019 Dec;7(12):1048-1058. doi: 10.1016/S2213-2600(19)30366-2. Epub 2019 Nov 12.
New anti-tuberculosis regimens that are shorter, simpler, and less toxic than those that are currently available are needed as part of the global effort to address the tuberculosis epidemic. We aimed to investigate the bactericidal activity and safety profile of combinations of bedaquiline, pretomanid, moxifloxacin, and pyrazinamide in the first 8 weeks of treatment of pulmonary tuberculosis.
In this multicentre, open-label, partially randomised, phase 2b trial, we prospectively recruited patients with drug-susceptible or rifampicin-resistant pulmonary tuberculosis from seven sites in South Africa, two in Tanzania, and one in Uganda. Patients aged 18 years or older with sputum smear grade 1+ or higher were eligible for enrolment, and a molecular assay (GeneXpert or MTBDRplus) was used to confirm the diagnosis of tuberculosis and to distinguish between drug-susceptible and rifampicin-resistant tuberculosis. Patients who were HIV positive with a baseline CD4 cell count of less than 100 cells per uL were excluded. Patients with drug-susceptible tuberculosis were randomly assigned (1:1:1) using numbered treatment packs with sequential allocation by the pharmacist to receive 56 days of treatment with standard tuberculosis therapy (oral isoniazid, rifampicin, pyrazinamide, and ethambutol; HRZE), or pretomanid (oral 200 mg daily) and pyrazinamide (oral 1500 mg daily) with either oral bedaquiline 400 mg daily on days 1-14 then 200 mg three times per week (BPaZ) or oral bedaquiline 200 mg daily (BPaZ). Patients with rifampicin-resistant tuberculosis received 56 days of the BPaZ regimen plus moxifloxacin 400 mg daily (BPaMZ). All treatment groups were open label, and randomisation was not stratified. Patients, trial investigators and staff, pharmacists or dispensers, laboratory staff (with the exception of the mycobacteriology laboratory staff), sponsor staff, and applicable contract research organisations were not masked. The primary efficacy outcome was daily percentage change in time to sputum culture positivity (TTP) in liquid medium over days 0-56 in the drug-susceptible tuberculosis population, based on non-linear mixed-effects regression modelling of log (TTP) over time. The efficacy analysis population contained patients who received at least one dose of medication and who had efficacy data available and had no major protocol violations. The safety population contained patients who received at least one dose of medication. This study is registered with ClinicalTrials.gov, NCT02193776, and all patients have completed follow-up.
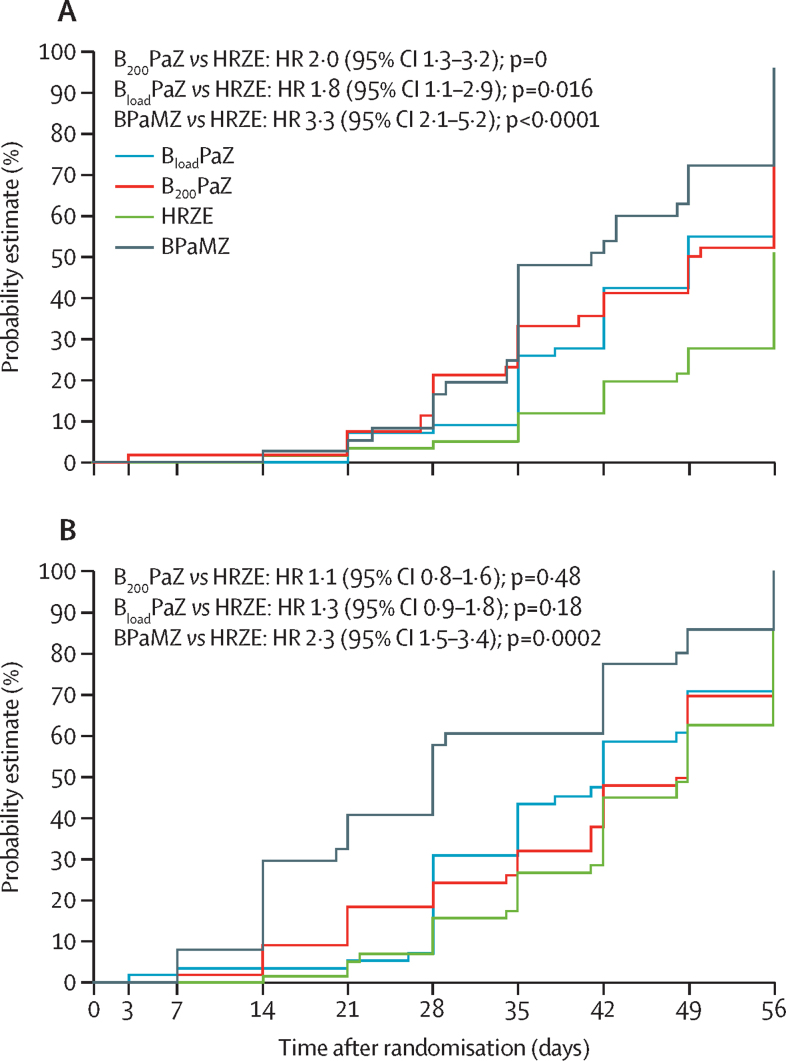
Between Oct 24, 2014, and Dec 15, 2015, we enrolled 180 patients with drug-susceptible tuberculosis (59 were randomly assigned to BPaZ, 60 to BPaZ, and 61 to HRZE) and 60 patients with rifampicin-resistant tuberculosis. 57 patients in the BPaZ group, 56 in the BPaZ group, and 59 in the HRZE group were included in the primary analysis. BPaZ produced the highest daily percentage change in TTP (5·17% [95% Bayesian credibility interval 4·61-5·77]), followed by BPaZ (4·87% [4·31-5·47]) and HRZE group (4·04% [3·67-4·42]). The bactericidal activity in BPaZ and BPaZ groups versus that in the HRZE group was significantly different. Higher proportions of patients in the BPaZ (six [10%] of 59) and BPaZ (five [8%] of 60) groups discontinued the study drug than in the HRZE group (two [3%] of 61) because of adverse events. Liver enzyme elevations were the most common grade 3 or 4 adverse events and resulted in the withdrawal of ten patients (five [8%] in the BPaZ group, three [5%] in the BPaZ group, and two [3%] in the HRZE group). Serious treatment-related adverse events affected two (3%) patients in the BPaZ group and one (2%) patient in the HRZE group. Seven (4%) patients with drug-susceptible tuberculosis died and four (7%) patients with rifampicin-resistant tuberculosis died. None of the deaths were considered to be related to treatment.
BPaZ is a promising regimen to treat patients with drug-susceptible tuberculosis. The bactericidal activity of both these regimens suggests that they have the potential to shorten treatment, and the simplified dosing schedule of BPaZ could improve treatment adherence in the field. However, these findings must be investigated further in a phase 3 trial assessing treatment outcomes.
TB Alliance, UK Department for International Development, Bill & Melinda Gates Foundation, US Agency for International Development, Directorate General for International Cooperation of the Netherlands, Irish Aid, Australia Department of Foreign Affairs and Trade, and the Federal Ministry for Education and Research of Germany.
目前,我们需要开发比现有药物更短、更简单、毒性更小的新型抗结核药物,作为全球应对结核病流行的一部分。我们旨在研究贝达喹啉、普托马尼德、莫西沙星和吡嗪酰胺联合治疗方案在治疗肺结核的前 8 周的杀菌活性和安全性。
在这项多中心、开放性标签、部分随机、2b 期临床试验中,我们前瞻性地招募了来自南非 7 个地点、坦桑尼亚 2 个地点和乌干达 1 个地点的药物敏感或利福平耐药肺结核患者。年龄在 18 岁或以上、痰涂片等级为 1+或更高的患者有资格入组,并且采用分子检测(GeneXpert 或 MTBDRplus)来确诊结核病并区分药物敏感和利福平耐药结核病。基线 CD4 细胞计数低于 100 个细胞/μL 的 HIV 阳性患者被排除在外。药物敏感肺结核患者随机(1:1:1)分组,药剂师通过编号治疗包进行顺序分配,接受标准肺结核治疗(口服异烟肼、利福平、吡嗪酰胺和乙胺丁醇;HRZE)或普托马尼德(口服 200 mg 每日)和吡嗪酰胺(口服 1500 mg 每日),联合口服贝达喹啉 400 mg 每日(第 1-14 天),然后每周 3 次 200 mg(BPaZ)或口服贝达喹啉 200 mg 每日(BPaZ)。利福平耐药肺结核患者接受 56 天的 BPaZ 方案加莫西沙星 400 mg 每日(BPaMZ)。所有治疗组均为开放性标签,且随机分组未分层。患者、试验研究者和工作人员、药剂师或药剂员、实验室工作人员(除分枝杆菌实验室工作人员外)、赞助商工作人员和适用的合同研究组织均未设盲。主要疗效终点是药物敏感肺结核人群中第 0-56 天液体培养阳性时间的每日百分比变化(TTP),基于时间对数 TTP 的非线性混合效应回归模型进行分析。疗效分析人群包含至少接受一剂药物且具有疗效数据且无重大方案违规的患者。安全性人群包含至少接受一剂药物的患者。本研究在 ClinicalTrials.gov 注册,NCT02193776,所有患者均已完成随访。
在 2014 年 10 月 24 日至 2015 年 12 月 15 日期间,我们纳入了 180 例药物敏感肺结核患者(59 例随机分为 BPaZ 组,60 例随机分为 BPaZ 组,61 例随机分为 HRZE 组)和 60 例利福平耐药肺结核患者。在主要分析中,57 例 BPaZ 组、56 例 BPaZ 组和 59 例 HRZE 组患者被纳入分析。BPaZ 组的 TTP 每日百分比变化最高(5.17%[95%贝叶斯可信度区间 4.61-5.77]),其次是 BPaZ 组(4.87%[4.31-5.47])和 HRZE 组(4.04%[3.67-4.42])。BPaZ 和 BPaZ 组与 HRZE 组相比,杀菌活性有显著差异。BPaZ(6 例[10%])和 BPaZ(5 例[8%])组中因不良事件停止研究药物的患者比例高于 HRZE 组(2 例[3%])。肝酶升高是最常见的 3 级或 4 级不良事件,导致 10 名患者停药(BPaZ 组 5 例[8%],BPaZ 组 3 例[5%],HRZE 组 2 例[3%])。BPaZ 组和 HRZE 组各有 1 例(2%)严重治疗相关不良事件。7 例(4%)药物敏感肺结核患者死亡,4 例(7%)利福平耐药肺结核患者死亡。没有死亡被认为与治疗有关。
BPaZ 是一种有前途的治疗药物敏感型肺结核的方案。这两种方案的杀菌活性表明它们有可能缩短治疗时间,并且 BPaZ 的简化给药方案可能会提高现场治疗的依从性。然而,这些发现必须在评估治疗结果的 3 期试验中进一步研究。
TB 联盟、英国国际发展部、比尔和梅琳达盖茨基金会、美国国际开发署、荷兰国际合作发展署、爱尔兰援助署、澳大利亚外交和贸易部以及德国联邦教育和研究部。