Peters Lilian, de Jonge Ank, de Boer Michiel, Downe Soo, Dahlen Hannah G
Department of Primary and Long-term Care, University of Groningen, University Medical Center, Groningen, The Netherlands
Western Sydney University, School of Nursing and Midwifery, Penrith, New South Wales, Australia.
BMJ Open. 2025 Jan 28;15(1):e086212. doi: 10.1136/bmjopen-2024-086212.
In this descriptive study, we aimed to assess how the index mode of birth and subsequent birth modes vary over time for public and private hospital maternity care funding models. The second aim was to determine to what extent the index mode of birth predicts subsequent birth modes in general and whether this differs in public versus private hospital maternity care funding models. With our aim, we have an innovative approach, specifically the women's life course approach, which is hypothesis-generating and can be assessed in future studies.
DESIGN, SETTING AND PARTICIPANTS: New South Wales population-linked data of low-risk women were analysed (2001-2016). Demographics and public/private care were recorded. Modes of the index birth and subsequent modes of second and third births (ie, spontaneous vaginal, instrumental vaginal elective/emergency caesarean birth) were registered. For those with 2 births and 3 births, 16 and 64 subsequent births patterns were created.
Trend of index modes of birth and subsequent modes of birth over time and the prediction of subsequent birth modes based on the index birth. These outcomes were stratified for the initial maternity care funding model.
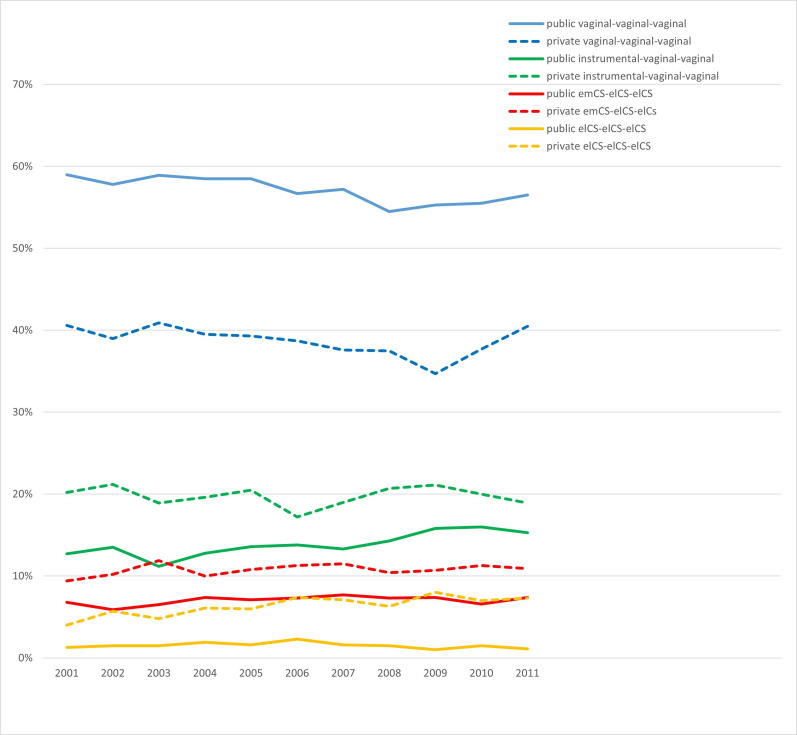
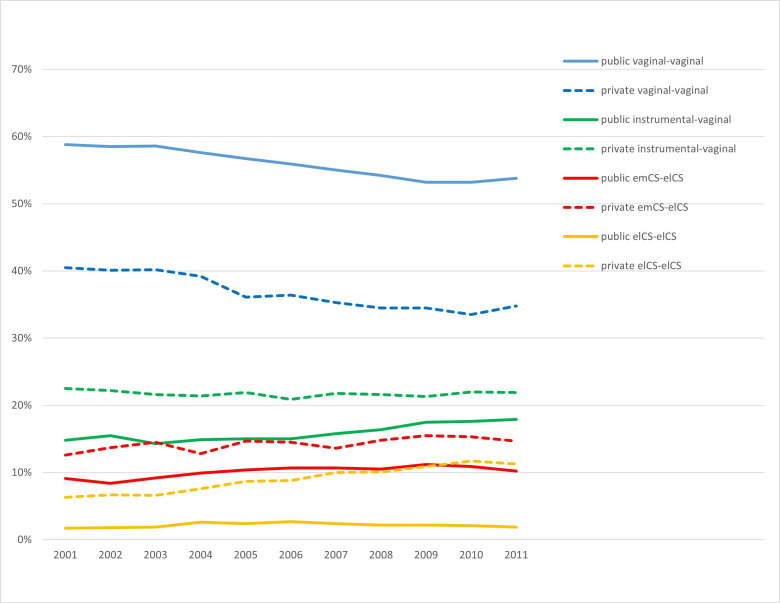
In total, 172 041 low-risk nulliparous women were included in the initial cohort, 54.1% had a spontaneous index vaginal birth and 71% had their index birth in public hospitals. During the study period, 131 675 women had 2 births and 44 677 of these women had 3 births, respectively. Among women birthing in public hospitals, higher proportions of index and subsequent vaginal births were observed than in private hospitals, with fewer instrumental vaginal births and caesarean sections. Large differences were observed for birth patterns: vaginal-vaginal (public 55.8% vs private 36.8%) and vaginal-vaginal-vaginal (public 57.2% vs private 38.8%). Women with an index spontaneous vaginal birth showed a high probability (91.3%) of subsequent spontaneous vaginal births. When stratified by maternity care funding model, the probabilities were similar: 91.6% in public hospitals and 90.2% in private hospitals.
Our study of low-risk Australian women (2001-2011) found that those giving birth in public hospitals had higher proportions of spontaneous vaginal births compared with private hospitals, where caesarean sections were more common. Women with an index spontaneous vaginal birth had a very high probability to have subsequent vaginal births. These findings suggest that index mode of birth may be a predictor for subsequent modes of birth.
在这项描述性研究中,我们旨在评估公立医院和私立医院产科护理资助模式下,首次分娩方式及后续分娩方式随时间的变化情况。第二个目的是确定首次分娩方式在多大程度上能预测后续一般分娩方式,以及在公立医院和私立医院产科护理资助模式下这一情况是否存在差异。基于我们的目的,我们采用了一种创新方法,即女性生命历程方法,该方法可生成假设,并可在未来研究中进行评估。
设计、设置和参与者:分析了新南威尔士州低风险女性的人口关联数据(2001 - 2016年)。记录了人口统计学信息及公立/私立护理情况。登记了首次分娩方式以及第二次和第三次分娩的后续方式(即自然阴道分娩、器械助产阴道分娩、择期/急诊剖宫产)。对于有两次分娩和三次分娩的女性,分别创建了16种和64种后续分娩模式。
首次分娩方式及后续分娩方式随时间的变化趋势,以及基于首次分娩对后续分娩方式的预测。这些结局按初始产科护理资助模式进行分层。
初始队列共纳入172041名低风险初产妇,54.1%的产妇首次自然阴道分娩,71%在公立医院进行首次分娩。在研究期间,分别有131675名女性生育两次,其中44677名女性生育三次。在公立医院分娩的女性中,首次及后续阴道分娩的比例高于私立医院,器械助产阴道分娩和剖宫产较少。在分娩模式上观察到很大差异:阴道 - 阴道(公立医院55.8%对私立医院36.8%)和阴道 - 阴道 - 阴道(公立医院57.2%对私立医院38.8%)。首次自然阴道分娩的女性后续自然阴道分娩的概率很高(91.3%)。按产科护理资助模式分层后,概率相似:公立医院为91.6%,私立医院为90.2%。
我们对澳大利亚低风险女性(2001 - 2011年)的研究发现,与剖宫产更常见的私立医院相比,在公立医院分娩的女性自然阴道分娩的比例更高。首次自然阴道分娩的女性后续阴道分娩的概率非常高。这些发现表明首次分娩方式可能是后续分娩方式的一个预测指标。