Johnson Jennifer E, Wiltsey-Stirman Shannon, Sikorskii Alla, Miller Ted, Poleshuck Ellen, Simas Tiffany A Moore, Carravallah Laura, Miller Raven, Zlotnick Caron
Charles Stewart Mott Department of Public Health, Michigan State University, 200 East 1st St Room 366, Flint, MI, 48502, USA.
National Center for PTSD, Department of Psychiatry and Behavioral Sciences, Dissemination and Training Division and Stanford University, 795 Willow Road (NC-PTSD 334), Menlo Park, CA, 94025, USA.
Implement Sci. 2025 Feb 10;20(1):9. doi: 10.1186/s13012-025-01420-z.
This Sequential Multiple Assignment Randomized Trial (SMART) was conducted to determine minimum implementation support needed for agencies serving pregnant people on public assistance to adopt and sustain the ROSE (Reach Out, Stay Strong, Essentials for mothers of newborns) postpartum depression (PPD) prevention program.
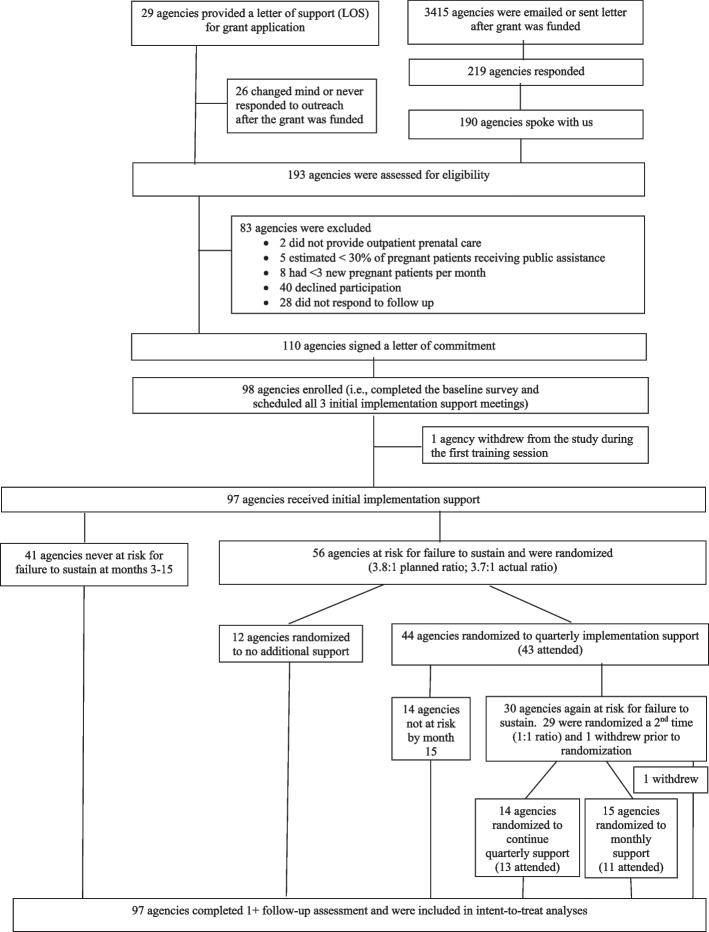
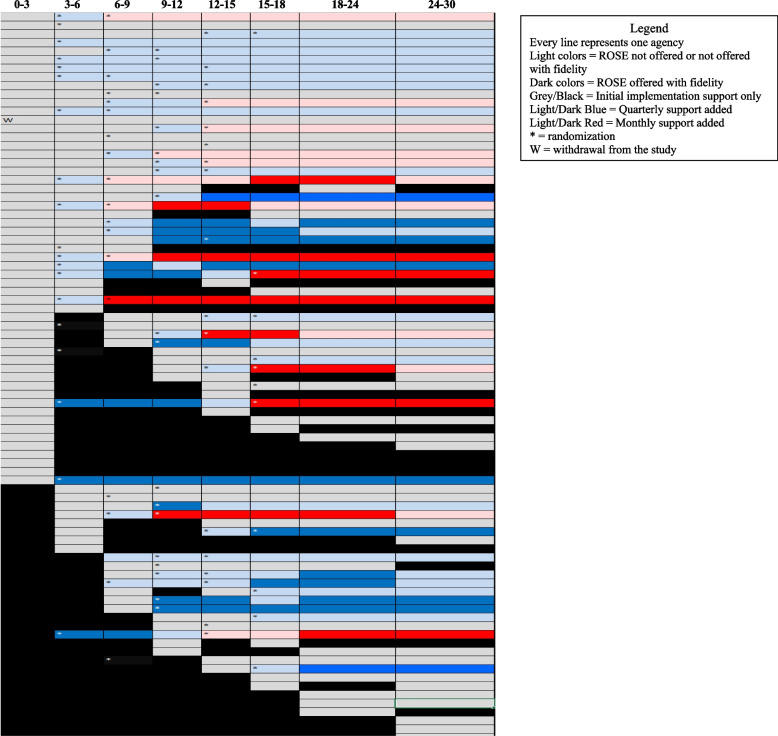
Enrolled prenatal agencies (N=98) received thorough initial implementation support (initial training + written sustainment planning). Agencies were identified as at risk for non-sustainment within the first 15 months (N=56) were randomized to: (1) no additional implementation support (N=12), or (2) quarterly implementation support (coaching and feedback; N=44). If agencies receiving quarterly implementation supports were still at risk and within the first 15 months (N=29), they were randomized to: (1) continued quarterly support (N=14), or (2) monthly implementation support (N=15). No implementation support occurred after 18 months. Follow-ups occurred quarterly and then at 18, 24, and 30 months. Outcomes included sustainment of core program elements, agency PPD rates, reach, and costs/cost-effectiveness of each sustainment step.
Twice as many agencies as expected (41 of 98; 42%) delivered ROSE with fidelity for 15+ months after receiving thorough initial implementation support only. For agencies at risk for non-sustainment, no effects of adding quarterly implementation supports were observed. However, adding monthly supports (versus quarterly) for agencies still at risk resulted in higher monthly percent of core ROSE elements sustained and more months ROSE was sustained with fidelity with large (Cohen's d = 0.73 and 0.80) effect sizes, and improved reach over 30 months. Many agencies did not consistently collect PPD rates, making results difficult to interpret. Mean implementation costs (including implementation support and agency staff time) per agency were $1,849 (SD $1,429) for agencies receiving initial implementation support only, $2,699 (SD $1,837) for those receiving initial and quarterly implementation support, and $4,059 (SD $1,763) for those receiving initial, quarterly, and ultimately monthly implementation support.
The cost of agency-wide ROSE implementation is far less than the cost of a single untreated case of PPD ($33,484). We suggest implementing ROSE through thorough training and written sustainment planning. For agencies not sustaining, adding monthly support can promote sustainment and improve reach.
Registered June 14, 2018 at clinicaltrials.gov, NCT03267563 ( https://clinicaltrials.gov/study/NCT03267563 ).
本序贯多重分配随机试验(SMART)旨在确定为接受公共援助的孕妇提供服务的机构采用并维持ROSE(伸出援手、保持坚强、新生儿母亲必备)产后抑郁症(PPD)预防项目所需的最低实施支持。
登记的产前机构(N = 98)接受了全面的初始实施支持(初始培训 + 书面维持计划)。被确定在最初15个月内有无法维持风险的机构(N = 56)被随机分为:(1)无额外实施支持(N = 12),或(2)季度实施支持(指导和反馈;N = 44)。如果接受季度实施支持的机构在最初15个月内仍有风险(N = 29),则将其随机分为:(1)继续季度支持(N = 14),或(2)月度实施支持(N = 15)。18个月后不再提供实施支持。随访每季度进行一次,然后在18、24和30个月时进行。结果包括核心项目要素的维持情况、机构PPD发生率、覆盖范围以及每个维持步骤的成本/成本效益。
仅接受全面初始实施支持后,实现ROSE保真度达15个月及以上的机构数量是预期的两倍(98个中的41个;42%)。对于有无法维持风险的机构,未观察到增加季度实施支持的效果。然而,对于仍有风险的机构增加月度支持(与季度支持相比),导致核心ROSE要素每月维持的百分比更高,ROSE保真度维持的月数更多,效应量较大(科恩d值 = 0.73和0.80),并在30个月内改善了覆盖范围。许多机构未持续收集PPD发生率,导致结果难以解释。仅接受初始实施支持的机构每个机构的平均实施成本(包括实施支持和机构工作人员时间)为1849美元(标准差1429美元),接受初始和季度实施支持的机构为2699美元(标准差1837美元),接受初始、季度并最终接受月度实施支持的机构为4059美元(标准差1763美元)。
全机构实施ROSE的成本远低于单个未治疗的PPD病例的成本(33484美元)。我们建议通过全面培训和书面维持计划来实施ROSE。对于无法维持的机构,增加月度支持可促进维持并改善覆盖范围。
于2018年6月14日在clinicaltrials.gov注册,NCT03267563(https://clinicaltrials.gov/study/NCT03267563)