Stapley Victoria, Anderson Roger S, Saunders Kathryn, Mulholland Pádraig J
Centre for Optometry and Vision Science, Biomedical Sciences Research Institute, Ulster University, Coleraine, UK.
National Institute for Health and Care Research (NIHR) Biomedical Research Centre at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, UK, London, UK.
Ophthalmic Physiol Opt. 2025 May;45(3):666-680. doi: 10.1111/opo.13460. Epub 2025 Feb 13.
Previous research suggests that the electroretinogram (ERG) is reduced and delayed in non-pathological myopia. However, the invasive nature of the electrode and cumbersome equipment required has prevented the widescale uptake of ERG measures. This study investigated whether previously reported changes to the ERG response in myopia are also observable when measured using non-invasive skin electrodes and a hand-held ERG device.
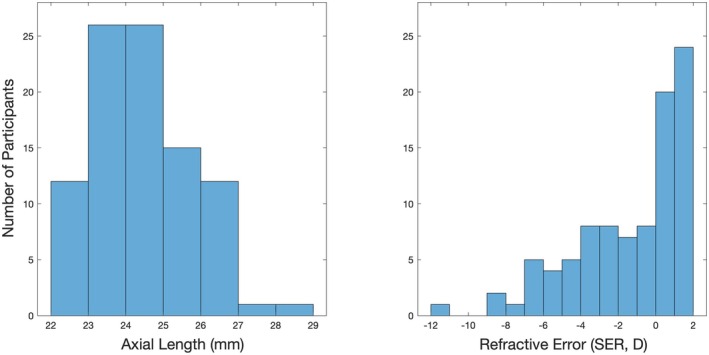
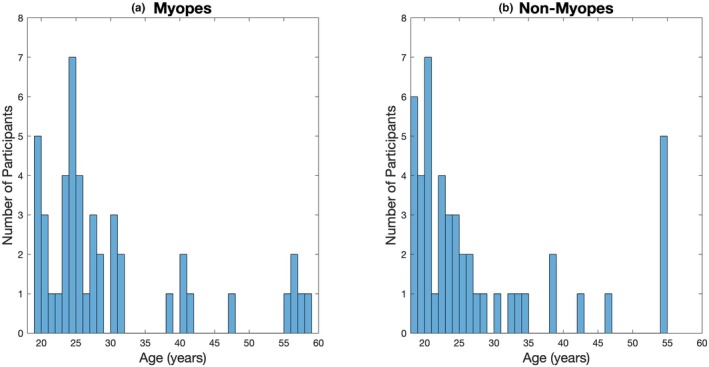
Monocular flash ERGs were measured using the RETeval® device according to the 'ISCEV 6 Step Dark First cd' protocol in 46 participants with non-pathological myopia (spherical equivalent refraction [SER] -0.50 to -11.25 D, median -3.75 D, median axial length [AL] 25.4 mm) and 47 non-myopic controls (SER +2.00 to -0.25 D, median +1.00 D, median AL 23.6 mm). Measures were performed under pupil mydriasis with Sensor Strip skin electrodes.
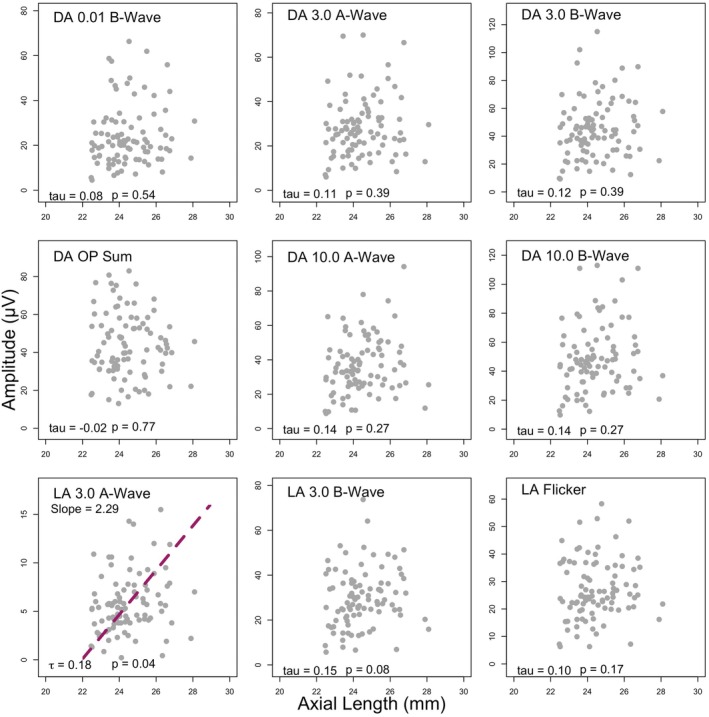
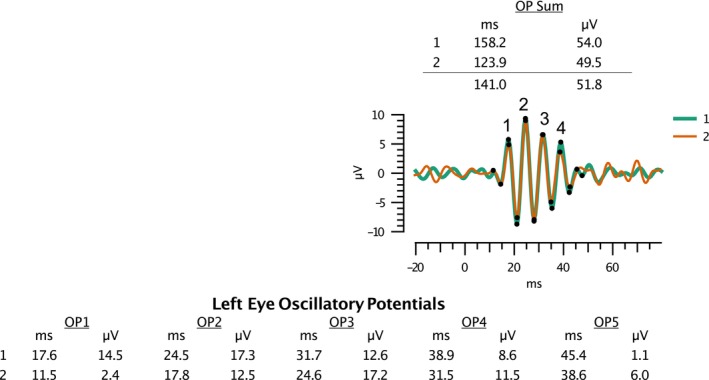
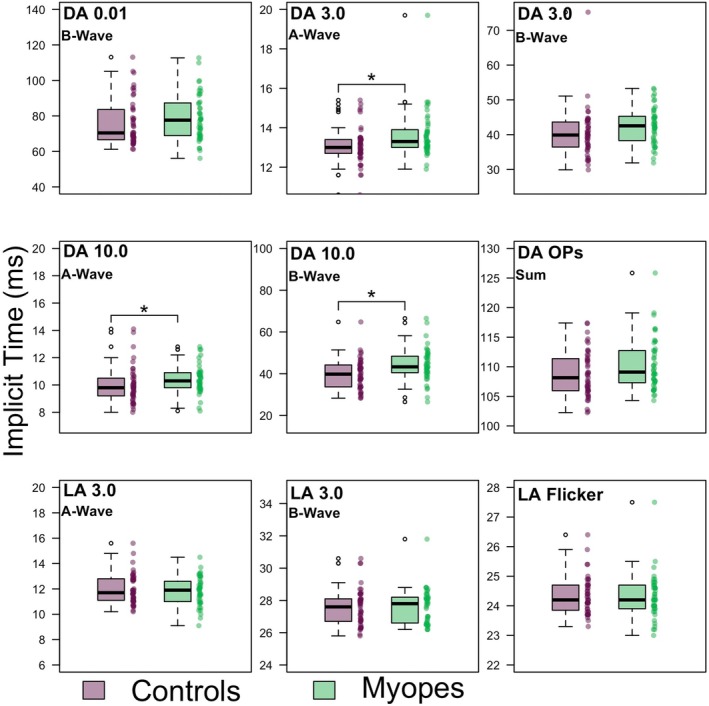
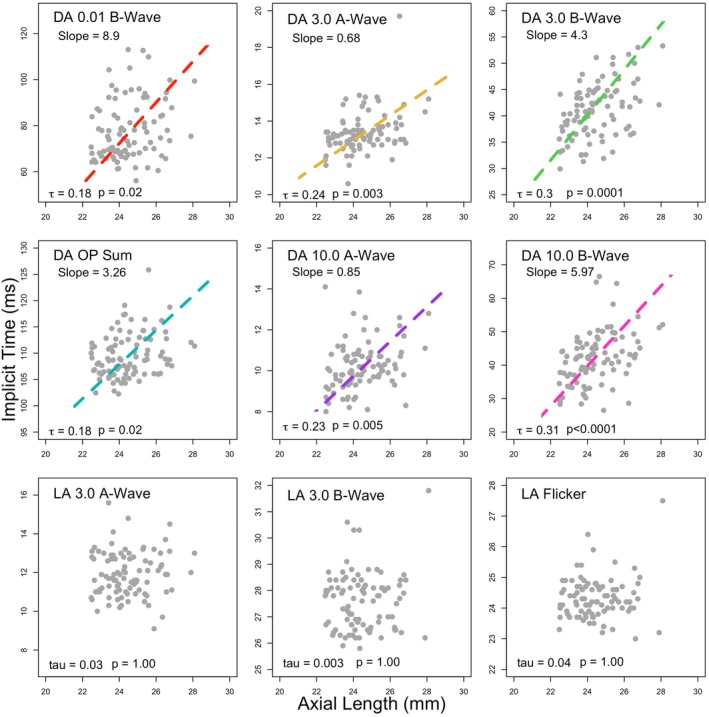
The median implicit time for all dark-adapted (DA) components was longer among myopes. Following Holm-Bonferroni correction, this difference reached statistical significance (p < 0.05) for the DA 3.0 A-wave, DA 10.0 A-wave and B-waves, and DA Oscillatory potentials 1 and 2. There were no significant differences between median light-adapted (LA) implicit times nor response amplitudes between refractive groups. For all DA components, there was a significant, positive correlation between AL and implicit time (all p < 0.05).
The RETeval®, used with skin electrodes, did not detect the reduction in ERG amplitude reported in myopic eyes using traditional ERG setups, potentially due to high inter-subject variability and/or anatomical confounders associated with the use of a skin electrode. The RETeval® with skin electrodes did detect subtle delays to DA implicit times previously reported in myopia, with a positive relationship observed between AL and implicit time for all DA components. In contrast, no significant differences were observed for LA implicit times, which may indicate underlying differences in the dark-adaptation process and/or scotopic visual pathways in myopia.
先前的研究表明,非病理性近视患者的视网膜电图(ERG)降低且延迟。然而,电极的侵入性以及所需设备的繁琐阻碍了ERG测量方法的广泛应用。本研究调查了使用非侵入性皮肤电极和手持式ERG设备进行测量时,近视患者中先前报道的ERG反应变化是否也可观察到。
根据“ISCEV 6步暗适应优先cd”方案,使用RETeval®设备对46名非病理性近视患者(等效球镜度[SER] -0.50至-11.25 D,中位数-3.75 D,眼轴长度[AL]中位数25.4 mm)和47名非近视对照者(SER +2.00至-0.25 D,中位数+1.00 D,AL中位数23.6 mm)进行单眼闪光ERG测量。测量在瞳孔散大状态下使用传感器条皮肤电极进行。
近视患者中所有暗适应(DA)成分的中位潜伏时间更长。经过Holm-Bonferroni校正后,DA 3.0 A波、DA 10.0 A波和B波以及DA振荡电位1和2的这种差异达到统计学显著性(p < 0.05)。不同屈光组之间的中位明适应(LA)潜伏时间和反应幅度均无显著差异。对于所有DA成分,AL与潜伏时间之间存在显著的正相关(所有p < 0.05)。
与皮肤电极一起使用的RETeval®未检测到使用传统ERG设置时报道的近视眼ERG幅度降低,这可能是由于个体间变异性高和/或与使用皮肤电极相关的解剖学混杂因素。带有皮肤电极的RETeval®确实检测到了先前报道的近视患者DA潜伏时间的细微延迟,并且所有DA成分的AL与潜伏时间之间存在正相关关系。相比之下,LA潜伏时间未观察到显著差异,这可能表明近视患者暗适应过程和/或暗视觉通路存在潜在差异。