Yilmaz Sule, Aryal Komal, King Jasmine, Bischof Jason J, Hong Arthur S, Wood Nancy, Gould Rothberg Bonnie E, Hudson Matthew F, Heinert Sara W, Wattana Monica K, Coyne Christopher J, Reyes-Gibby Cielito, Todd Knox, Lyman Gary, Klotz Adam, Abar Beau, Grudzen Corita, Bastani Aveh, Baugh Christopher W, Henning Daniel J, Bernstein Steven, Rico Juan Felipe, Ryan Richard J, Yeung Sai-Ching Jim, Qdaisat Aiham, Padela Aasim, Madsen Troy E, Liu Raymond, Adler David
Division of Palliative Care, Department of Medicine, University of Rochester Medical Center, 265 Crittenden Blvd., Rochester, NY, 14642, USA.
McMaster University, Hamilton, ON, Canada.
BMC Emerg Med. 2025 Mar 5;25(1):40. doi: 10.1186/s12873-025-01183-2.
Patients with cancer frequently visit the emergency department (ED) and are at high risk for hospitalization due to severe illness from cancer progression or treatment side effects. With an aging population and rising cancer incidence rates worldwide, it is crucial to understand how EDs and other acute care venues manage oncologic emergencies. Insights from other nations and health systems may inform resources necessary for optimal ED management and novel care delivery pathways. We described clinical management of oncologic emergencies and their contribution to ED visits and hospitalizations worldwide.
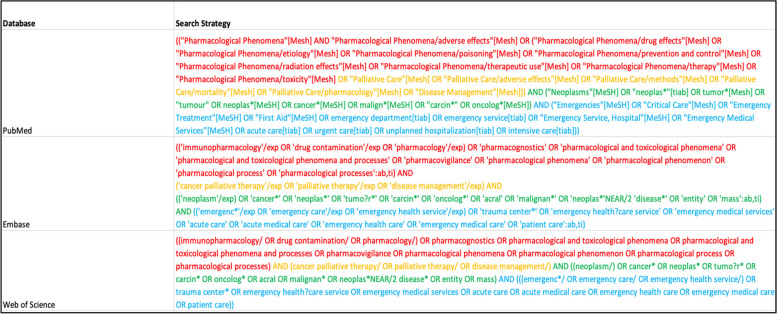
We performed a systematic review of peer-reviewed original research studies published in the English language between January 1st, 2003, to December 31st, 2022, garnered from PubMed, Web of Science, and EMBASE. We included all studies investigating adult (≥ 18 years) cancer patients with emergency visits. We examined chief complaints or predictors of ED use that explicitly defined oncologic emergencies.
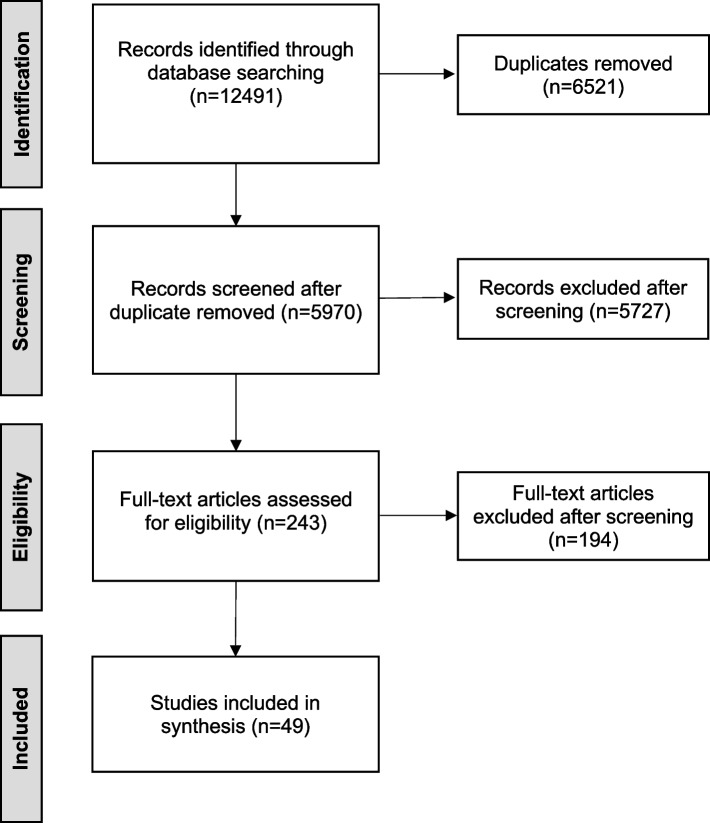
The search strategy yielded 49 articles addressing cancer-related emergency visits. Most publications reported single-site studies (n = 34/49), with approximately even distribution across clinical settings- ED (n = 22/49) and acute care hospital/ICU (n = 27/49). The number of patient observations varied widely among the published studies (range: 9 - 87,555 patients), with most studies not specifying the cancer type (n = 33/49), stage (n = 41/49), or treatment type (n = 36/49). Most studies (n = 31/49) examined patients aged ≥ 60 years. Infection was the most common oncologic emergency documented (n = 22/49), followed by pain (n = 20/49), dyspnea (n = 19/49), and gastrointestinal (GI) symptoms (n = 17/49). Interventions within the ED or hospital ranged from pharmacological management with opioids (n = 11/49), antibiotics (n = 9/49), corticosteroids (n = 5/49), and invasive procedures (e.g., palliative stenting; n = 13/49) or surgical interventions (n = 2/49).
Limited research specifically addresses oncologic emergencies despite the international prevalence of ED presentations among cancer patients. Patients with cancer presenting to the ED appear to have a variety of complaints which could result from their cancers and thus may require tailored diagnostic and intervention pathways to provide optimal acute care. Further acute geriatric oncology research may clarify the optimal management strategies to improve the outcomes for this vulnerable patient population.
癌症患者经常前往急诊科(ED),由于癌症进展或治疗副作用导致的严重疾病,他们住院风险很高。随着全球人口老龄化和癌症发病率上升,了解急诊科和其他急性护理场所如何管理肿瘤急症至关重要。其他国家和卫生系统的见解可能为优化急诊科管理和新型护理提供途径所需的资源提供信息。我们描述了肿瘤急症的临床管理及其对全球急诊科就诊和住院的影响。
我们对2003年1月1日至2022年12月31日期间以英文发表的同行评审原创研究进行了系统综述,这些研究来自PubMed、科学网和EMBASE。我们纳入了所有调查成年(≥18岁)癌症患者急诊就诊情况的研究。我们检查了明确界定肿瘤急症的急诊科使用的主要投诉或预测因素。
检索策略产生了49篇关于癌症相关急诊就诊的文章。大多数出版物报告的是单中心研究(n = 34/49),在临床环境中的分布大致均匀——急诊科(n = 22/49)和急性护理医院/重症监护室(n = 27/49)。已发表研究中的患者观察数量差异很大(范围:9 - 87,555名患者),大多数研究未明确癌症类型(n = 33/49)、分期(n = 41/49)或治疗类型(n = 36/49)。大多数研究(n = 31/49)调查的是年龄≥60岁的患者。感染是记录到的最常见的肿瘤急症(n = 22/49),其次是疼痛(n = 20/49)、呼吸困难(n = 19/49)和胃肠道(GI)症状(n = 17/49)。急诊科或医院内的干预措施包括使用阿片类药物(n = 11/49)、抗生素(n = 9/49)、皮质类固醇(n = 5/49)进行药物管理,以及侵入性操作(如姑息性支架置入;n = 13/49)或手术干预(n = 2/49)。
尽管癌症患者在急诊科就诊在国际上很普遍,但专门针对肿瘤急症的研究有限。前往急诊科的癌症患者似乎有各种各样的投诉,这可能是由他们的癌症引起的,因此可能需要量身定制的诊断和干预途径以提供最佳的急性护理。进一步的急性老年肿瘤学研究可能会阐明改善这一脆弱患者群体结局的最佳管理策略。