Scherer Karin Antonia, Büdenbender Björn, Blum Anja K, Grüne Britta, Kriegmair Maximilian C, Michel Maurice S, Alpers Georg W
Department of Psychology, School of Social Sciences, University of Mannheim, Mannheim, Germany.
Department of Urology and Urosurgery, Medical Faculty Mannheim, University Medical Center Mannheim, Heidelberg University, Mannheim, Germany.
BMC Med Inform Decis Mak. 2025 Mar 10;25(1):120. doi: 10.1186/s12911-025-02938-4.
Shared decision-making (SDM) is the gold standard for patient-clinician interaction, yet many patients are not actively involved in medical consultations and hesitate to engage in decisions on their health. Despite considerable efforts to improve implementation, research on barriers to SDM within the patient-clinician relationship and interaction is scant. To identify potential barriers to urological patients' participation in decision-making, we developed two novel scales assessing power asymmetry (PA-ME) and embarrassment in medical encounters (EmMed). The present study validates both scales in a large sample comprising urological patients and non-clinical participants. It further examines the effects of both factors on participation preferences and decisional conflict among patients.
Data were collected from 107 urological patients at a university hospital for Urology and Urosurgery in Germany. Patients completed self-report questionnaires before and after their clinical appointments. In addition, 250 non-clinical participants provided data via an online study. All participants rated perceived power asymmetry in the patient-clinician relationship and their experience of embarrassment in medical contexts using the PA-ME and EmMed scales. Urological patients further indicated their participation preference in decisions regarding both general and urological care prior to the consultation. Afterward, they assessed the level of perceived decisional conflict.
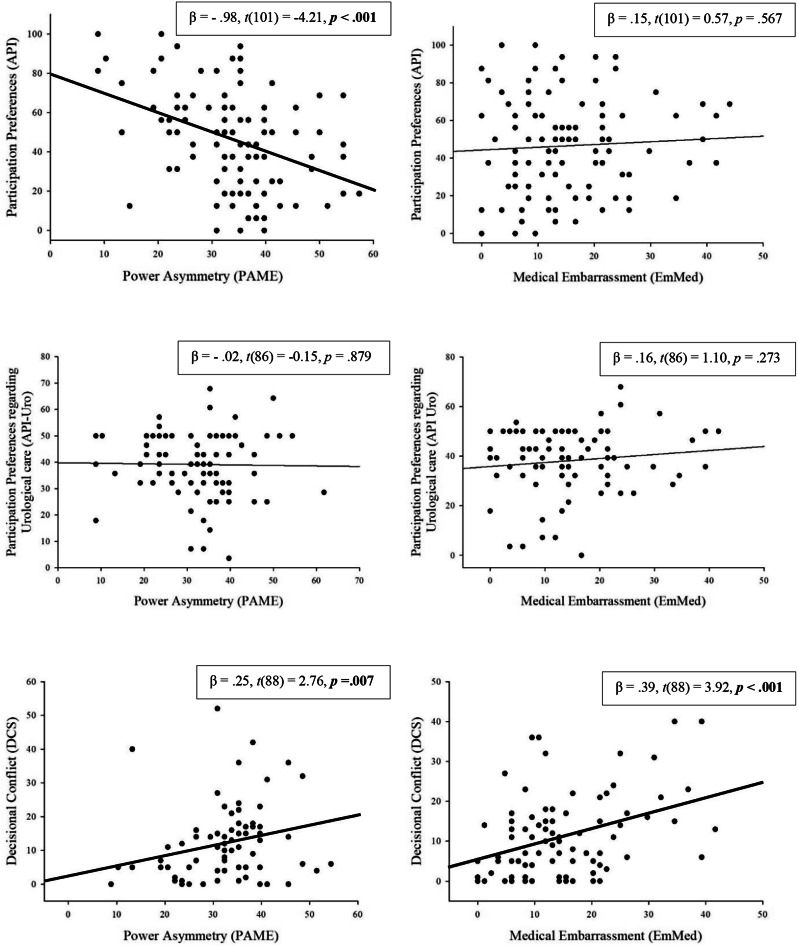
Factor analyses yielded power asymmetry and medical embarrassment as unidimensional constructs. Both questionnaires have good (PA-ME; α = 0.88), respectively excellent (EmMed; α = 0.95), internal consistency. Among urological patients, higher levels of perceived power asymmetry predicted lower generic participation preference (β = - 0.98, p <.001, adjusted R = 0.14) and higher decisional conflict (β = 0.25, p <.01, adjusted R = 0.07). While, in patients, embarrassment was not linked to generic participation preference before the consultation (p ≥.5), it resulted in higher decisional conflict after the consultation (β = 0.39, p <.001, adjusted R = 0.14). Neither power asymmetry nor embarrassment were specifically associated with participation preference regarding urological care (p ≥.273).
Given their promising psychometric properties, the new instruments are recommended for routine assessment of power asymmetry and embarrassment among patients. Addressing these factors may be helpful to reduce decisional conflict and increase participation preferences. Both factors are prerequisites for a successful SDM-process and active patient engagement in health-related decisions.
共同决策(SDM)是患者与临床医生互动的黄金标准,但许多患者并未积极参与医疗咨询,并且在参与自身健康决策时犹豫不决。尽管为改善实施情况付出了巨大努力,但关于患者与临床医生关系及互动中共同决策障碍的研究却很少。为了确定泌尿外科患者参与决策的潜在障碍,我们开发了两个新量表,分别评估权力不对称(PA - ME)和医疗互动中的尴尬感(EmMed)。本研究在一个包含泌尿外科患者和非临床参与者的大样本中验证了这两个量表。它还进一步研究了这两个因素对患者参与偏好和决策冲突的影响。
数据收集自德国一家大学医院泌尿外科和泌尿外科手术科室的107名泌尿外科患者。患者在临床预约前后完成自我报告问卷。此外,250名非临床参与者通过在线研究提供数据。所有参与者使用PA - ME和EmMed量表对患者与临床医生关系中感知到的权力不对称以及他们在医疗环境中的尴尬经历进行评分。泌尿外科患者在咨询前还需表明他们对一般医疗护理和泌尿外科护理决策的参与偏好。之后,他们评估感知到的决策冲突程度。
因素分析得出权力不对称和医疗尴尬是单维结构。两个问卷分别具有良好的(PA - ME;α = 0.88)和出色的(EmMed;α = 0.95)内部一致性。在泌尿外科患者中,较高水平的感知权力不对称预示着较低的一般参与偏好(β = - 0.98,p <.001,调整后R = 0.14)和较高的决策冲突(β = 0.25,p <.01,调整后R = 0.07)。虽然在患者中,尴尬感在咨询前与一般参与偏好无关(p≥.5),但在咨询后导致了较高的决策冲突(β = 0.39,p <.001,调整后R = 0.14)。权力不对称和尴尬感均与泌尿外科护理的参与偏好无特定关联(p≥.273)。
鉴于其良好的心理测量特性,建议将这两个新工具用于常规评估患者中的权力不对称和尴尬感。解决这些因素可能有助于减少决策冲突并提高参与偏好。这两个因素都是成功的共同决策过程以及患者积极参与健康相关决策的先决条件。