Muwonge Joseph Junior, Jablonska Beata, Dalman Christina, Burström Bo, Galanti Maria Rosaria, Hollander Anna-Clara
Department of Global Public Health, Karolinska Institute, Stockholm, Sweden.
Centre for Epidemiology and Community Medicine, Stockholm Health Care Services, Region Stockholm, Stockholm, Sweden.
Int J Equity Health. 2025 Apr 8;24(1):98. doi: 10.1186/s12939-025-02453-y.
Horizontal equity is defined as equal care for equal needs, regardless of socioeconomic factors. This study investigated trends in horizontal equity in mental health care (MHC) utilization in Sweden from 2006 to 2022. Monitoring equity provides valuable information for healthcare system governance (e.g., planning and resource allocation) necessary for ensuring equitable provision of services.
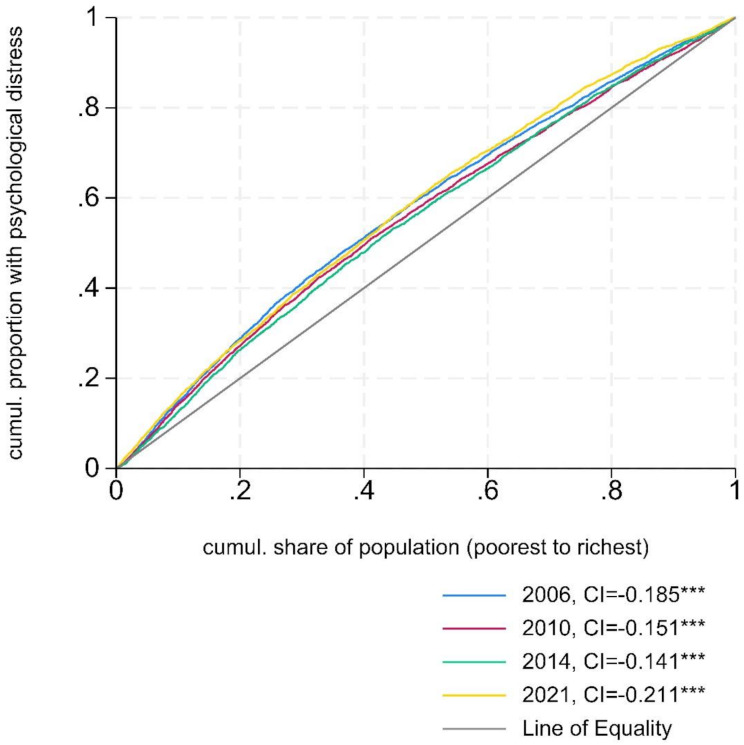
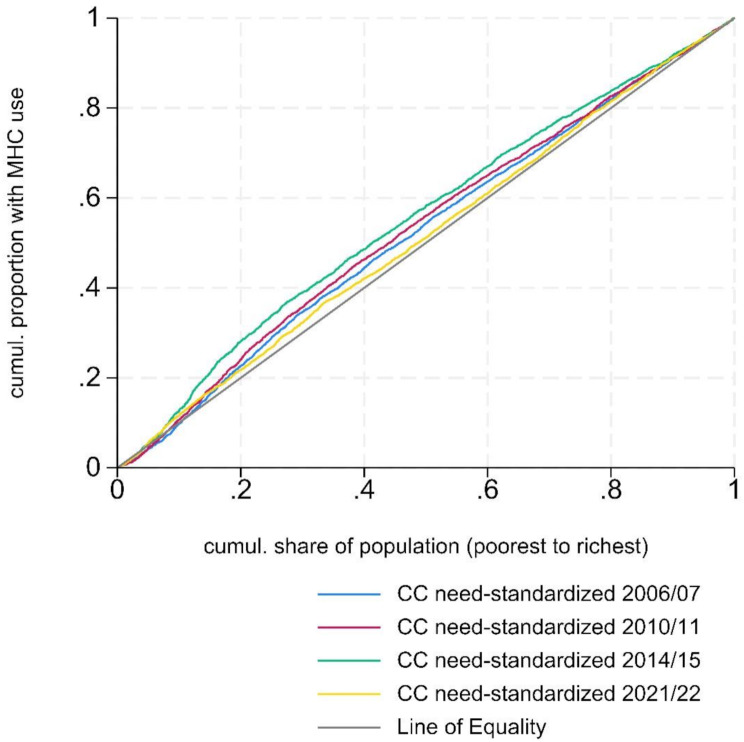
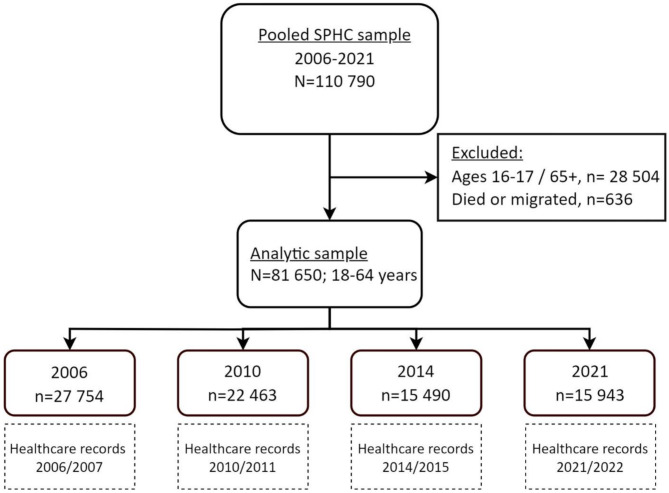
A total of 81,650 Stockholm residents aged 18-64, who participated in the Hälsa Stockholm surveys of 2006, 2010, 2014 or 2021, were analysed. Their subsequent use of MHC (primary, in- and outpatient specialized care, and psychotropic medication) within six months after survey response was collected from registries between 2006 and 2022. Concentration index (CI) and need-standardized CI (Horizontal inequity index, HI), summative measures of inequalities, were used in this study. HI was estimated using self-reported psychological distress (measured with the General health questionnaire 12 in 2006-2014 and Kessler 6 in 2021) as the primary need indicator, with general health status and long-term limiting illness as additional need indicators. Equivalized disposable household income was used as the ranking variable, while education status, migration status, age, and sex were included as non-need variables that we controlled for in the analyses.
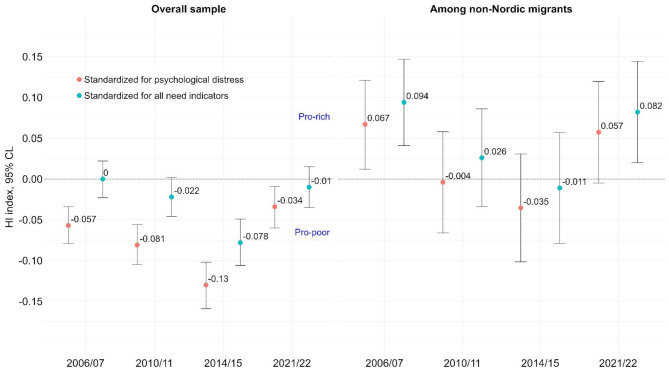
Lower-income individuals used MHC services more than their higher-income counterparts with comparable levels of psychological distress. These "pro-poor" inequities in the probability of MHC use increased from HI = -0.057 [95% Confidence Limits, CL: -0.079, -0.034] in 2006/2007 to HI = -0.130 [95% CL: -0.159, -0.102] in 2014/2015. By 2021/2022, the "pro-poor" inequities had decreased (HI = -0.034 [95% CL: -0.06, -0.009]), partly due to an increase in MHC use among higher-income groups but a decrease in the lowest income group. Standardizing for additional need indicators reduced the "pro-poor" inequities but maintained the observed trends. Among non-Nordic migrants, "pro-rich" inequities fell between 2006/2007 and 2014/2015 but rose in 2021/2022, with significant "pro-rich" inequities among non-European migrants in 2021/2022 (HI = 0.100 [95% CL: 0.024, 0.176]). Among patients in outpatient services, "pro-poor" inequities in visit frequency decreased over time (2006-2022).
We observed increasingly higher probability of MHC use among lower-income individuals than their higher-income peers with similar (measured) needs from 2006 to 2015. However, during the pandemic (2021/2022), potential access problems led to diminishing of "pro-poor" inequities in the total sample, and to "pro-rich" inequities among non-Nordic migrants. The Covid-19 disruption to the healthcare system-such as restrictions on in-person visits and the rapid transition to digital healthcare services-along with its impact on care-seeking, may explain the trend shifts.
横向公平被定义为不论社会经济因素,对同等需求给予同等的医疗服务。本研究调查了2006年至2022年瑞典心理健康护理(MHC)利用方面的横向公平趋势。监测公平性为医疗系统治理(如规划和资源分配)提供了有价值的信息,这对于确保公平提供服务是必要的。
对2006年、2010年、2014年或2021年参与斯德哥尔摩健康调查的81650名18 - 64岁的斯德哥尔摩居民进行了分析。从2006年至2022年的登记处收集了他们在调查回复后六个月内对MHC(初级、住院和门诊专科护理以及精神药物)的后续使用情况。本研究使用了不平等的汇总指标——集中指数(CI)和需求标准化CI(横向不平等指数,HI)。HI是使用自我报告的心理困扰(2006 - 2014年用一般健康问卷12测量,2021年用凯斯勒6项量表测量)作为主要需求指标进行估计的,一般健康状况和长期限制性生活疾病作为额外的需求指标。等效可支配家庭收入用作排序变量,而教育状况、移民身份、年龄和性别作为非需求变量纳入分析并加以控制。
在心理困扰程度相当的情况下,低收入个体比高收入个体更多地使用MHC服务。这些在MHC使用概率方面的“有利于穷人”的不平等现象从2006/2007年的HI = -0.057 [95%置信区间,CL:-0.079,-0.034]增加到2014/2015年的HI = -0.130 [95% CL:-0.159,-0.102]。到2021/2022年,“有利于穷人”的不平等现象有所减少(HI = -0.034 [95% CL:-0.06,-0.009]),部分原因是高收入群体中MHC使用增加,而最低收入群体中使用减少。对额外需求指标进行标准化减少了“有利于穷人”的不平等现象,但保持了观察到的趋势。在非北欧移民中,“有利于富人”的不平等现象在2006/2007年至201,4/2015年期间有所下降,但在2021/2022年有所上升,2021/2022年非欧洲移民中存在显著的“有利于富人”的不平等现象(HI = 0.100 [95% CL:0.024,0.176])。在门诊患者中,就诊频率方面“有利于穷人”的不平等现象随时间推移而减少(2006 - 2022年)。
我们观察到,从2006年到2015年,低收入个体比具有相似(测量的)需求的高收入同龄人使用MHC的概率越来越高。然而,在大流行期间(2021/2022年),潜在的获取问题导致总样本中“有利于穷人”的不平等现象减少,以及非北欧移民中出现“有利于富人”的不平等现象。新冠疫情对医疗系统的干扰——如对面对面就诊的限制以及向数字医疗服务的快速转变——以及其对就医行为的影响,可能解释了这种趋势变化。