Singh Jasvinder A, Hearld Larry R, Eisen Seth, Chatham W Winn, Narain Sonali, Annapureddy Narender, Kamen Diane L, Trotter Kimberly, Majithia Vikas, Lee Ching Cathy, Aouhab Zineb, Venuturupalli Swamy, Wallace Daniel J, Ramsey-Goldman Rosalind, Kim Alfred, McMahon Maureen, Sam Lim S, Bhairavarasu Kalpana, Meara Alexa, Kalunian Kenneth, Beasley T Mark
Medicine Service, Michael E. DeBakey VA Medical Center, Houston, TX, USA.
Department of Medicine, Baylor College of Medicine, Houston, TX, USA.
Rheumatology (Oxford). 2025 Aug 1;64(8):4631-4640. doi: 10.1093/rheumatology/keaf205.
The objective of this study was to examine the clinical outcomes during the implementation of a self-administered patient decision-aid (PtDA) for lupus.
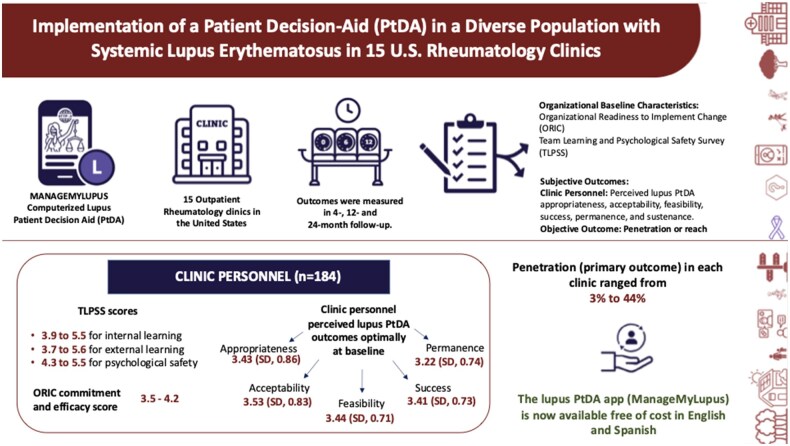
We provided an effective computerized lupus PtDA in 15 rheumatology outpatient clinics 2019-2024 (including the COVID pandemic). We undertook Organizational Readiness to Implement Change Surveys (ORICs) and Team Learning and Psychological Safety Surveys (TLPSSs) at baseline. The primary study outcome objective measure, percent penetration/reach, was defined as the number of patients who viewed the lupus PtDA at the end of the study, divided by the total number of eligible patients (times 100). We used validated clinical personnel surveys to examine the perceived lupus PtDA appropriateness, acceptability, feasibility, success, and permanence, at 4 months, 12 months and 24 months post-PtDA implementation.
Among the sites, the clinical personnels' (n = 184) baseline ORIC commitment and efficacy scores (a 0-5 scale, higher = better) ranged from 3.5 to 4.2, and 3.4 to 4.4, respectively; the TLPSS scores (a 0-7 scale, higher = better) were 3.9-5.5 for internal learning, 3.7-5.6 for external learning, and 4.3-5.5 for psychological safety. The penetration (primary outcome) among 15 geographically diverse US rheumatology clinics ranged from 3% to 44%. We found that the total number of providers in the clinic was positively associated with higher penetration. Clinical personnel-perceived lupus PtDA outcomes were optimal at 4 months (all scale scores ranged from 1 to 5, higher = better): (i) appropriateness, 3.43 (s.d. 0.86); (ii) acceptability, 3.53 (s.d. 0.83); (iii) feasibility, 3.44 (s.d. 0.71); (iv) success, 3.41 (s.d. 0.73); and (v) permanence, 3.22 (s.d. 0.74).
We implemented a lupus PtDA with varied success rates during the COVID pandemic; more providers were associated with higher clinic penetration. Clinical personnel perceived high lupus PtDA appropriateness, acceptability, feasibility, success, and permanence that persisted up to 24 months.
ClinicalTrials.gov, http://clinicaltrials.gov, NCT03735238.
本研究的目的是检验针对狼疮的患者自我管理决策辅助工具(PtDA)实施过程中的临床结果。
2019年至2024年期间(包括新冠疫情期间),我们在15个风湿病门诊提供了有效的计算机化狼疮PtDA。我们在基线时进行了组织变革准备度调查(ORIC)和团队学习与心理安全调查(TLPSS)。主要研究结果的客观指标,即渗透率/覆盖率百分比,定义为研究结束时查看狼疮PtDA的患者数量除以符合条件的患者总数(乘以100)。我们使用经过验证的临床人员调查问卷,在PtDA实施后的4个月、12个月和24个月,检查对狼疮PtDA的适用性、可接受性、可行性、成功率和持久性的认知。
在各研究点中,临床人员(n = 184)的基线ORIC承诺和效能得分(0至5分制,分数越高越好)分别为3.5至4.2和3.4至4.4;TLPSS得分(0至7分制,分数越高越好)中,内部学习为3.9至5.5,外部学习为3.7至5.6,心理安全为4.3至5.5。美国15个地理位置不同的风湿病诊所的渗透率(主要结果)在3%至44%之间。我们发现诊所内提供者的总数与较高的渗透率呈正相关。临床人员对狼疮PtDA结果的认知在4个月时最佳(所有量表得分范围为1至5分,分数越高越好):(i)适用性,3.43(标准差0.86);(ii)可接受性,3.53(标准差0.83);(iii)可行性,3.44(标准差0.71);(iv)成功率,3.41(标准差0.73);(v)持久性,3.22(标准差0.74)。
在新冠疫情期间,我们实施了狼疮PtDA,成功率各不相同;更多的提供者与更高的诊所渗透率相关。临床人员认为狼疮PtDA具有较高的适用性、可接受性、可行性、成功率和持久性,这种情况持续了24个月。
ClinicalTrials.gov,http://clinicaltrials.gov,NCT03735238